3444
Liver and muscle energy metabolism in patients with organic acidemias using 31P and 1H MR spectroscopy1Institute for Clinical Diabetology, German Diabetes Center, Leibniz Institute for Diabetes Research, Heinrich Heine University, Duesseldorf, Germany, 2German Center for Diabetes Research (DZD e.V.), Partner Düsseldorf, Duesseldorf, Germany, 3Experimental Pediatrics and Metabolism, University Children’s Hospital, Heinrich Heine University, Duesseldorf, Germany, 4Institute for Biometrics and Epidemiology, German Diabetes Center, Leibniz Institute for Diabetes Research, Heinrich Heine University, Duesseldorf, Germany, 55Department of Endocrinology and Diabetology, Medical Faculty, Heinrich Heine University, Duesseldorf, Germany
Synopsis
This study assessed energy and fat metabolism in a well phenotyped cohort of patients with organic acidemias using non-invasive MR spectroscopy. 31P and 1H spectra of the liver as well as 1H spectra of the muscle were acquired in 27 patients and 30 healthy controls (age-, sex-, BMI-matched). We found higher liver fat content in patients with propionic acidemia. The level of creatine in the soleus muscle was higher in patients with methylmalonic acidemia and propionic acidemia. In conclusion, the results provide evidence for previously unknown abnormalities of liver fat and muscle energy metabolism in patients with organic acidemias.
PURPOSE
Patients with organic acidemias accumulate amino acid derivatives as a result of disrupted branched-chain amino acid metabolism. This may lead to abnormal functioning of mitochondria, which can in turn affect carbohydrate and fat metabolism (1,2). Previous case studies employed biopsies from liver transplantats to investigate the hepatic proteome and used 1H MR spectroscopy to study brain metabolism (3–5). The aim of this case-control study was to assess energy and fat metabolism in a larger well phenotyped cohort using non-invasive MR spectroscopy.METHODS
27 children and young adults (6-34 years) with organic acidemias [14 with methylmalonic acidemia (MMA), 7 with propionic acidemia (PA) and 6 with isovaleric acidemia (IVA)] and 30 healthy humans (5-34 years), matched for age, sex and BMI to the respective disease group (CON 1,2,3,4), were studied on a clinical scanner (3T Philips Achieva, Best, The Netherlands). All participants consented to the protocol approved by the local ethics board prior to the study. The 14 MMA patients comprised of 8 patients with classic MMA and 6 patients with cobalamin A or B deficiency (Cbl A, Cbl B). 31P MR spectra were acquired using a 14 cm circular 31P surface coil (Philips Healthcare), with the 1H body coil for 1H-decoupling and NOE enhancement. Prior to 31P MRS acquisition, a 4×4×4 cm³ (children) or 6x5x6 cm³ (youth) voxel of interest was placed within the liver avoiding muscle. 3D localized liver spectra [TR=6 s, number of signal averages=128] were obtained using ISIS as described previously (1). Liver fat was quantified from non-water-suppressed 1H MR spectra using stimulated echo acquisition mode (STEAM) and absolute concentrations were expressed as per cent hepatocellular lipids relative to water content. Intramyocellular lipids (IMCL) were measured in the left soleus using FLEX-S coils (Philips Healthcare) and a single-voxel point-resolved spectroscopy (PRESS) sequence (TR/TE=2.000/32 ms). Post-processing of 31P/1H spectra in the liver was done with jMRUI (AMARES), IMCL was quantified using LCModel.RESULTS
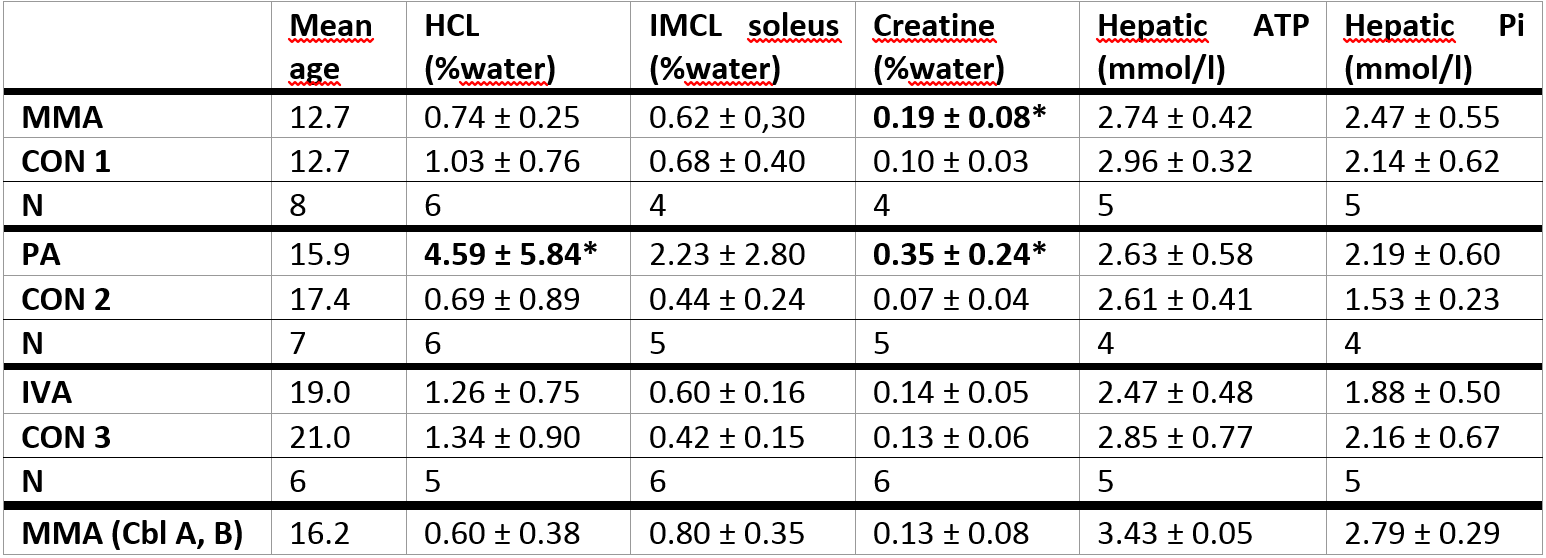
Due to the difficulty in compliance with the study procedure for pediatric and developmentally delayed participants, not all measurements could be performed in all patients and controls. The hepatic concentrations of ATP and Pi were not significantly different between patients with organic acidemias and healthy age-, sex- and BMI-matched controls. However, liver fat content (HCL) was higher in patients with PA (p=0.03). Also, the level of creatine in the soleus muscle was higher in both patients with MMA (p=0.05) and PA (p=0.03) (Table 1).DISCUSSION
This case-control study found higher levels of hepatocellular lipids in PA and of creatine in PA and MMA. The differences in energy and fat metabolism might be related to accumulating metabolites specific to the enzyme defect in branched-chain amino acid metabolism and/or due to a resulting lack of energy-supplying products. In line with the finding that, among the branched-chain organic acidemias, patients with PA generally are more severely affected (6), they also showed the most marked alterations in hepatic fat content and intramyocellular creatine accumulation in our analyses.CONCLUSION
This study shows that MR spectroscopy is also able to noninvasively detect alterations in liver and muscle metabolism of patients with branched-chain organic acidemias. The results provide evidence for previously unknown abnormalities of liver fat and muscle energy metabolism in a larger group of children, youth and young adults with different types of organic acidemias. These data thereby complement previously published case reports on altered brain metabolite concentrations (3,4) and structural changes (7). Even larger cohort studies are required to evaluate the role of the identified metabolic changes for the clinical phenotype and monitoring of treatment of these diseases.Acknowledgements
This work was supported by the Ministry of Innovation, Science and Research of the State of North Rhine-Westphalia and the German Federal Ministry of Health. This study was supported in part by a grant from the Federal Ministry of Education and Research (BMBF) to the German Center for Diabetes Research.References
1. Wilnai Y, Enns GM, Niemi A-K, Higgins J, Vogel H. Abnormal Hepatocellular Mitochondria in Methylmalonic Acidemia. Ultrastruct Pathol. 2014 Oct 1;38(5):309–14.
2. Chandler RJ, Zerfas PM, Shanske S, Sloan J, Hoffmann V, DiMauro S, et al. Mitochondrial dysfunction in mut methylmalonic acidemia. FASEB J Off Publ Fed Am Soc Exp Biol. 2009 Apr;23(4):1252–61.
3. Takeuchi M, Harada M, Matsuzaki K, Hisaoka S, Nishitani H, Mori K. Magnetic resonance imaging and spectroscopy in a patient with treated methylmalonic acidemia. J Comput Assist Tomogr. 2003 Aug;27(4):547–51.
4. Davison JE, Davies NP, Wilson M, Sun Y, Chakrapani A, McKiernan PJ, et al. MR spectroscopy-based brain metabolite profiling in propionic acidaemia: metabolic changes in the basal ganglia during acute decompensation and effect of liver transplantation. Orphanet J Rare Dis. 2011 May 9;6:19.
5. Caterino M, Chandler RJ, Sloan JL, Dorko K, Cusmano-Ozog K, Ingenito L, et al. The proteome of methylmalonic acidemia (MMA): the elucidation of altered pathways in patient livers. Mol BioSyst. 2016 Jan 26;12(2):566–74.
6. Nizon M, Ottolenghi C, Valayannopoulos V, Arnoux J-B, Barbier V, Habarou F, et al. Long-term neurological outcome of a cohort of 80 patients with classical organic acidurias. Orphanet J Rare Dis. 2013 Sep 23;8:148.
7. Bindu PS, Kovoor JME, Christopher R. Teaching NeuroImages: MRI in methylmalonic acidemia. Neurology. 2010 Jan 26;74(4):e14–e14.
Figures