3423
Feasibility of diffusion kurtosis imaging as a tool for differentiation between benign and malignant uterine lesions1Radiology, Kagoshima University Graduate School of Medical and Dental Sciences, Kagoshima, Japan, 2Radiological Technology, Kagoshima University Hospital, Kagoshima, Japan, 3Philips Electronics Japan, TN, Japan
Synopsis
This study focused on the feasibility of DKI for differentiating benign from malignant uterine lesions. The ADC and D of malignant tumor (MT) were significantly lower than those of endometrial hyperplasia (EH) (p=0.005 and 0.004), uterine fibroid (UF) (both, p<0.001), normal endometrium (NE) (both, p<0.001), and normal myometrium (NM) (both, p<0.001), which indicative of the increased cellularity within uterine malignant tumor that resulted in restricted water diffusion. K was significantly higher in MT than in EH (p=0.003), UF (p<0.001), NE (p<0.001), and NM (p<0.001), possibly representing
Purpose
The conventional DWI model is based on the assumption that water diffusion follows a Gaussian behavior such that water molecules diffuse without any restriction. While in living tissue, the diffusion is normally restricted by tissue microstructure and shows non-Gaussian phenomena (1). Diffusion kurtosis imaging (DKI) is sensitive to deviations from Gaussian diffusion behavior, and allows more robust characterization of the tissue diffusion (1). Recently, DKI parameters have been proved to be able to indicate microstructural characteristics within cerebral glioma, hepatocellular carcinoma, prostate cancer (2) and breast lesion (3). However, no study has demonstrated the utility of DKI for differential diagnosis in the uterine lesions. Therefore, the purpose of this study was to evaluate the feasibility of DKI for differentiating benign from malignant uterine lesions.Methods
Our study population consisted of 118 patients with histologically confirmed uterine lesions including 87 malignant tumors (MT) (49 endometrial carcinomas, 36 cervical cancers, and 2 carcinosarcomas), 7 endometrial hyperplasias (EH), and 24 uterine fibroids (UF). Diffusivity (D) and kurtosis (K) maps were calculated from DKI data obtained with b values of 0, 500, 1000, 1500, and 2000 /mm2. Apparent diffusion coefficient (ADC) map was generated using the images with b values of 0 and 1000 sec/mm2 from the same DKI data. ADC, D, and K in MT, EH, UF, as well as in the normal endometrium (NE) and myometrium (NM) were measured using a region of interest (ROI). ADC, D, and K of MT were compared with those of EH, UF, NE, and NM by using the Kruskal-Wallis test, followed by Steel test. ROC analysis was used to assess the ability of the ADC, D, and K to differentiate MT from benign lesions (EH and UF) and normal uterine tissues (NE and NM).Results
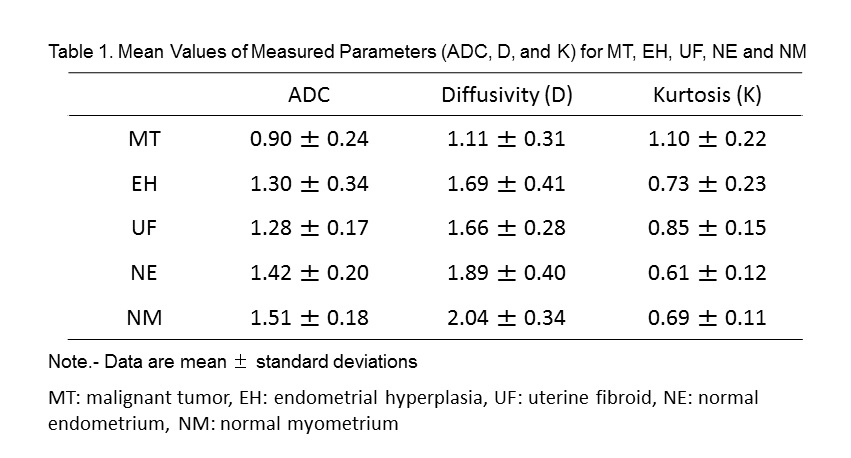
The results of ADC and DKI parameters are summarized in Table 1. ADC and D of MT were significantly lower than those of EH (p=0.005 and 0.004), UF (both, p<0.001), NE (both, p<0.001), and NM (both, p<0.001). K was significantly higher in MT than in EH (p=0.003), UF (p<0.001), NE (p<0.001), and NM (p<0.001). The areas under the ROC curve of D and K were 0.877 and 0.883 for differentiation from EH, 0.926 and 0.823 for UF, 0.955 and 0.969 for NE, and 0.976 and 0.942 for NM, respectively.Discussion
In this study, ADC of MT was significantly lower than those of benign lesions (EH, UF, NE, and NM), which are supported by previous studies showing that uterine malignant tumors (endometrial cancer and cervical cancer) have lower ADC than endometrial hyperplasia, uterine fibroid, normal endometrium, and normal myometrium. The D of MT was significantly lower than those of EH, UF, NE, and NM. The D, which is corrected for non-Gaussian diffusion behavior, has been reported to show similar behavior to ADC. Therefore, our lower D in uterine malignant tumor is agreement with the increased cellularity within uterine malignant tumor that resulted in restricted water diffusion. The K of MT was significantly higher than those of EH, UF, NE, and NM. It was reported that K was significantly higher for malignant than for benign lesions in the breast (2) and prostate (3). The K has been considered to be associated with complexity of tissue microstructure. Therefore, MT may have more heterogeneous tissue structures compared with benign lesions in the uterus.Conclusion
The results suggested that DKI might be useful for differentiation of malignant uterine lesions from benign lesions.Acknowledgements
No acknowledgement found.References
1. Jensen J, Helpern J, Ramani A, et al. Diffusion kurtosis imaging: the quantification of non-gaussian water diffusion by means of magnetic resonance imagning. Magn Reson Med 2005; 53:1432-1440
2. Rosenkrantz A, Prabhu V, Sigmund E, et al. Utitlity of diffusional kurtosis imaging as a marker of adverse pathologic outcomes among prostate cancer active surveillance candidates undergoing radical prostatectomy. AJR 2013; 201:840-846.
3. Kun S, Xiaosong C, Weimin C, et al. Breast cancer: Diffusion kurtosis MR imaging – diagnostic accuracy and correlation with clinical pathologic factors. Radiology 2015; 277:46-55.
Figures