3422
Use of texture analysis of intravoxel incoherent motion (IVIM) in evaluating the expression of Ki67 of hepatitis B virus-related hepatocellular carcinoma (HCC)1Department of Radiology, the Third Affiliated Hospital, Sun Yat-sen University (SYSU), Guangzhou, People's Republic of China, 2GE Healthcare MR Research China, Guangzhou, People's Republic of China, 3MR Research China,GE Healthcare, Beijing, 4Mayo Clinic
Synopsis
HCC is the second cause of cancer-related deaths and most HCC patients are accompanied with hepatitis B virus-related cirrhosis in China. Ki67 is a protein reflecting the proliferative activity of HCC and could be used as a predictor of prognosis. We assessed the value of the texture parameters in evaluating the expression of Ki67of HBV-related HCCs by whole tumor analysis. Our results showed that Dclusterprominence showed best diagnostic performance among all texture parameters. ADC and IVIM derived texture parameters might be used as useful and noninvasive biomarkers for evaluating the expression of Ki67 of HBV-related HCCs.
Introduction
Hepatocellular carcinoma (HCC) is the most common primary malignancy of the liver worldwide1.Surgery resection and liver transplantation have been considered the only curative treatments. However, the prognosis remains still poor due to the high rate of recurrence. Ki67 is a protein which reflects the proliferative activity of HCC. High expression of Ki67 is a strong predictor of recurrence and poor prognosis in HCC patients after surgery2,3.Intravoxel incoherent motion (IVIM) has been used for evaluating histologic grade of HCC4, assessing therapeutic effect and predicting prognosis5,6.However, the utility of evaluating the expression of Ki67 using IVIM in HBV-related HCCs is not clear. This study aimed to evaluate the value of IVIM texture parameters in predicting the expression of Ki67in HBV-related HCCs.Methods
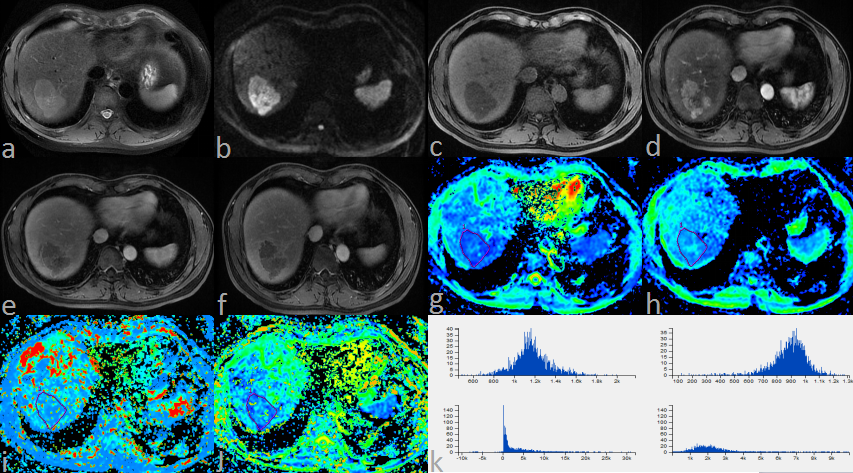
The study was approved by the institutional review board of our hospital and 154 patients with chronic HBV infection who were diagnosed with HCC pathologically after surgical resection or liver transplantation were included initially. 93 patients were excluded: (a) 18 received previous transarterial chemoembolization (TACE), (b) 11 had no lesion larger than 1cm in size, (c) 2 had distinct motion artifacts and 6 had slice misregistration, (d) 56 did not have available information on the expression of Ki67. A total of 61 patients (53 males and 8 females; age range, 25-75 years; mean, 54 years)with 61 HCCs were enrolled finally. In patients with multiple tumors, the largest one was analyzed. Immunohistochemistry was used to test the expression of Ki67.Ki-67 of 10% was considered positive expression. The patients were classified into two groups: Ki67 positive (n=48) and Ki67 negative (n=13). All subjects underwent MRI exam on a 3.0T whole-body MRI scanner (Discovery MR750, GE Healthcare, Milwaukee, WI). Respiratory-triggered diffusion-weighted imaging (DWI) were performed using 11 b values (b=0, 30, 50, 100, 150, 200, 300, 500, 800, 1000, 1500 sec/mm2).Regions of interests (ROIs) were manually placed on each axial image of ADC maps to encompass as much lesion as possible using T2W images as a reference. Afterwards, volumes of interests (VOIs) which encompass the whole tumor were generated automatically by summing all ROIs using a manufacturer developed tool (Omni-Kinetics, GE Healthcare). The VOIs were then transferred to other parameter maps automatically. Apparent diffusion coefficient (ADC), diffusion coefficient (D), pseudodiffusion coefficient (D*) and perfusion fraction (f) derived texture parameters of the HCCs were calculated based on histogram and grey level co-occurrence matrix (GLCM) algorithm7. The differences between the Ki67 (+) and Ki67 (-) group were compared using the Student t test or Mann-Whitney test according to the statistical distribution of the data. Receiver operating characteristic (ROC) analysis was performed to assess the diagnostic performance of these parameters for evaluating the expression of Ki67 of HCCs.Results
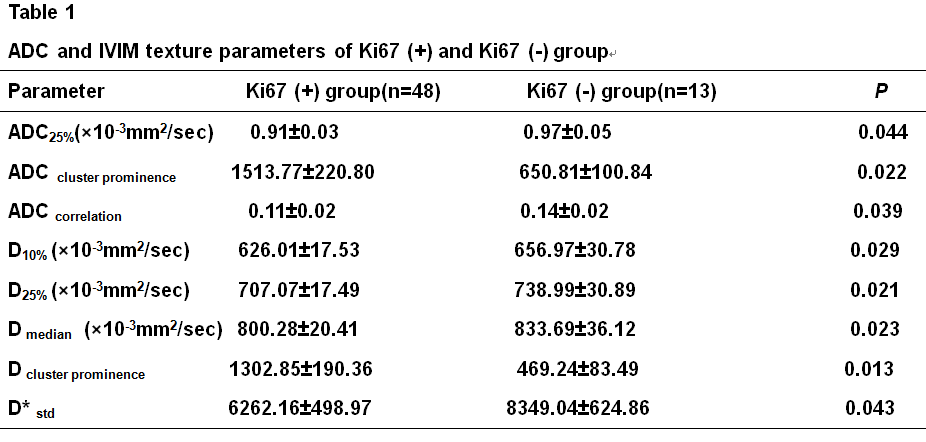
ADCcluster prominence and Dcluster prominence, of the Ki67(+) group were significantly higher than those of Ki67(-) group (P=0.022 and 0.013, respectively). ADC25%,ADCcorrelation,Dmedian,D10% and D25% of the Ki67(+) group were significantly lower than those of the Ki67(-) group ( P=0.044, 0.039, 0.023,0.029 and 0.021, respectively). The area under the ROC curve (AUC-ROC) of the above texture parameters in predicting the positive expression Ki67 was 0.708, 0.726, 0.65, 0.688, 0.67, 0.663 and 0.672, respectively.Discussion
In this study, ADC and IVIM texture parameters of the whole tumor were calculated. Texture analysis could reflect the tumor heterogeneity and the whole tumor analysis might provide a better approach for extracting information of tumors7.Our study showed that the ADC and IVIM derived texture parameters have the potential value for predicting the expression of Ki67 of HBV-related HCCs. According to ROC analysis, Dclusterprominence showed best diagnostic performance among all texture parameters. However, the AUC of texture parameters was relatively low, which might be due to the small sample size. Larger sample size and prospective studies are further needed to investigate the value of texture parameters of ADC and IVIM as biomarkers for evaluating the expression of Ki67 of HBV-related HCC.Conclusion
In summary, texture parameters of ADC and IVIM could be used as useful and noninvasive biomarkers for predicting the expression of Ki67 of HBV-related HCCs and might be helpful when selecting more appropriate treatment and predicting prognosis.Acknowledgements
NoReferences
1. de Martel C, Maucort-Boulch D, Plummer M, et al. World-wide relative contribution of hepatitis B and C viruses in hepatocellular carcinoma[J]. Hepatology,2015,62(4):1190-1200.
2. Mann C D, Neal C P, Garcea G, et al. Prognostic molecular markers in hepatocellular carcinoma: A systematic review[J]. Eur J Cancer,2007,43:979-992.
3. Qin L, Tang Z. The prognostic molecular markers in hepatocellular carcinoma[J]. World J Gastroenterol,2002,8:385-392.
4.Woo S, Lee J M, Yoon J H, et al. Intravoxel incoherent motion diffusion-weighted MR imaging of hepatocellular carcinoma: correlation with enhancement degree and histologic grade[J]. Radiology,2014,270:758-767.
5.Lewin M, Fartoux L, Vignaud A, et al. The diffusion-weighted imaging perfusion fraction f is a potential marker of sorafenib treatment in advanced hepatocellular carcinoma: a pilot study[J]. Eur Radiol,2011,21:281-290.
6.Park Y S, Lee C H, Kim J H, et al. Using intravoxel incoherent motion (IVIM) MR imaging to predict lipiodol uptake in patients with hepatocellular carcinoma following transcatheter arterial chemoembolization: A preliminary result[J]. MagnReson Imaging,2014,32:638-646.
7.Nougaret S, Vargas H A, Lakhman Y, et al. Intravoxel Incoherent Motion-derived Histogram Metrics for Assessment of Response after Combined Chemotherapy and Radiation Therapy in Rectal Cancer: Initial Experience and Comparison between Single-Section and Volumetric Analyses[J]. Radiology,2016,280:446-454.
Figures