3377
Two subgroups of mild TBI Patients Revealed by Diffusion TensorImaging and Cluster Analysis1Department of Biomedical Engineering, the Key Laboratory of Biomedical Information Engineering of the Ministry of Education, Xi'an Jiaotong University, Xi'an, People's Republic of China, 2Department of Linguistics, Xidian University, Xi'an, People's Republic of China, 3Center for Language and Brain, Shenzhen Institute of Neuroscience, Shenzhen University, shenzhen, People's Republic of China
Synopsis
More than 75% of traumatic brain injuries (TBI) seeking medical attention are mild, and the outcome of mild TBI (mTBI) is heterogeneous. Currently we are in badly need of the methods of classifying mTBI into more homogeneous subgroups since there is not a sensitive and valid biomarker identified right now. In current study, we aim to investigate whether different subgroups exist in a large cohort patients and to predict neuropsychological outcome in the future.
Introduction
Traumatic brain injury (TBI) is a critical public health and socio-economic problem throughout the world. Over 75% of TBI seeking medical attention are mild, and outcome in that group is heterogeneous[1]. However, little is known about the subgroups with homogeneous features. Several evidence support the hypothesis that TBI is associated with pathophysiological alterations in cerebral white matter. Clustering may be feasible to divide a large cohort into subgroups of TBI. The purpose of this study is to investigate whether there exist different subgroups in a large cohort patients and to predict neuropsychological outcome based on microstructural changes in white matter.Methods
This study was approved by the local institutional review board. Diffusion tensor imaging (DTI) was acquired by a single-shot, spin echo-based and diffusion-weighted echo planar imaging sequence on a 3T MRI scanner (Siemens Trio) (TR = 7300 ms; TE = 99 ms; b = 0, 1000 s/ mm2; gradient orientations number = 30; thickness = 3 mm; slices = 50; FOV = 256×256 mm2; matrix size = 128×128; two averages; voxel size = 2× 2 ×3 mm3). For routine DTI processing, head motion, eddy current correction, brain extraction and tensor model fitting were all performed using FSL[2] (FMRIB Software Library, FMRIB). After that,the FA feature,which is the diffusion measurement along the tract core, defined as the tract profile, was extracted from each fiber tract using JUH WM label atlas. In order to get an optimal feature combination which can split the mild TBI (mTBI) subgroups, agglomerative hierarchical clustering was performed on patients and controls using the white matter features in every possible combination[3]. The optimal cluster number was determined using Silhouette, Dunn, and connectivity indices, which reflect the compactness, separation, and connectedness of the generated clusters[3]. Besides, mTBI patients were divided into 2 groups using cognitive information processing speed (IPS), while the first group was equal to the control group, and the other was much bigger. At last, two IPS subgroups and hierarchical clustering results were matched to compute the accuracy. The same process was also operated in the 3-month follow-up mTBI group. At last, FA profiles were compared between healthy control individuals and patient subgroups in a pointwise manner using permutation-based statistical analysis with 5000 permutations using FSL (p<0.05 regarded as significant).Results
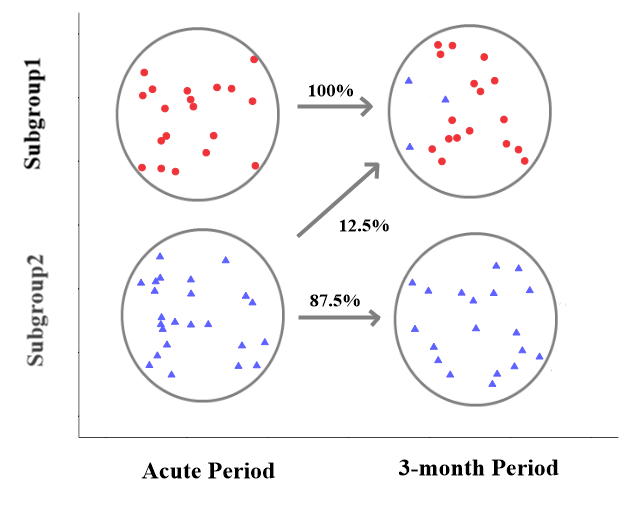
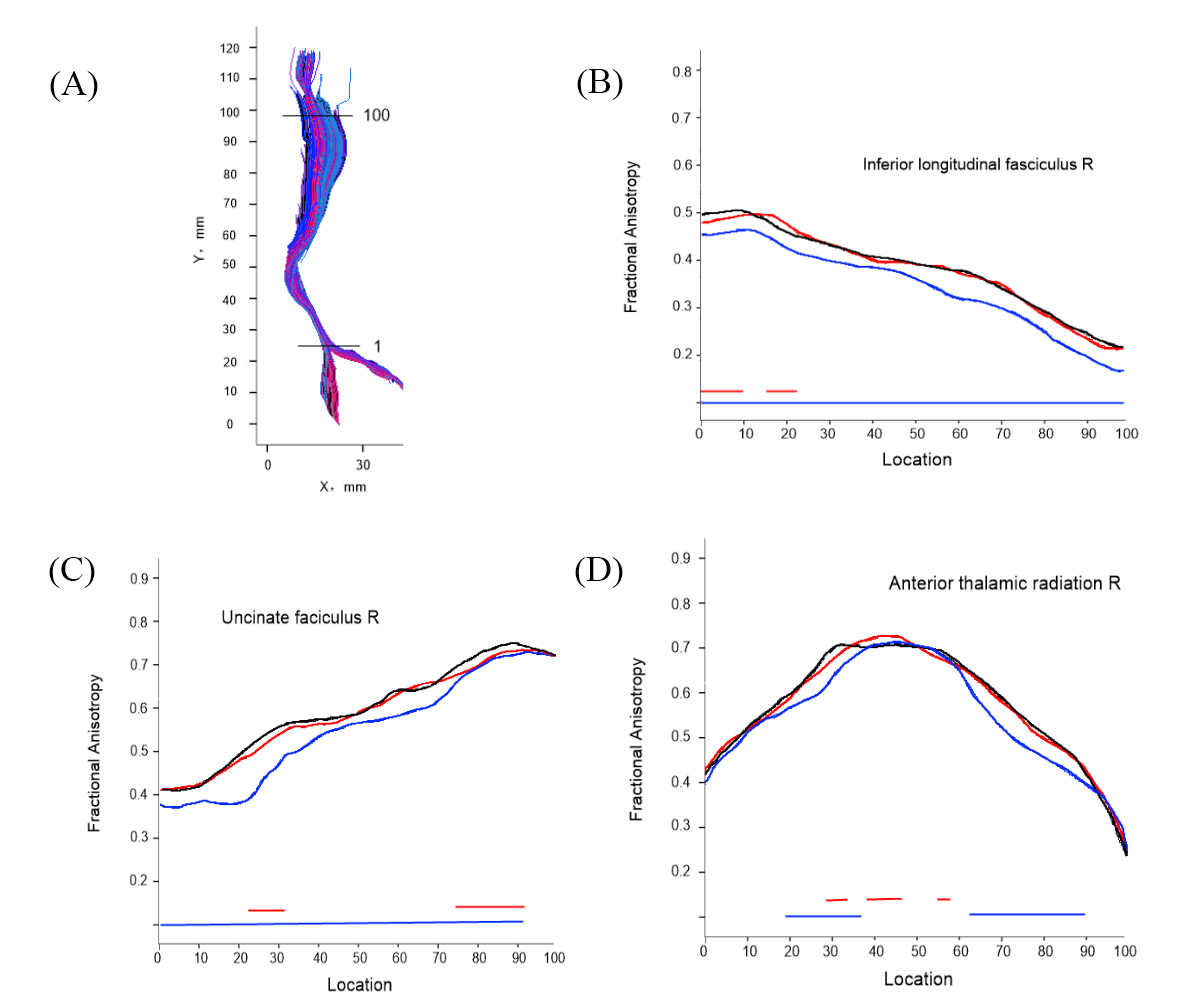
43 mTBI patients with mean age of 47±5 and 42 gender, age socio-cultural level matched controls were included in this study. Our cluster method achieved the best Silhouette (0.48), Dunn (20.15) and connectivity (2.56) when the cluster number was equal to 2. 8 white matter tracts were determined when identifying mTBI group from control group using hierarchical clustering with a high accuracy (>80%, p=0.026). Then, mTBI patients were divided into 2 subgroups in acute period (19 and 24 patients) and 3-month period (21 and 22 patients) separately with the 8 determined tracts. Taking the IPS as criterion, the accuracy of the clustering method was high (86%, p=0.031 and 87.5%, p=0.029 for acute and 3-month period, respectively). Comparing the clustering results between acute and 3-month period, we found that there were only 7% mTBI patients assigned in the wrong subgroup (Fig 1). In pointwise comparison of FA profiles, subgroup 2 showed widespread FA reduction relative control individuals in the right Inferior longitudinal fasciculus, right uncinated fasciculus, and right anterior thalamic radiation (Fig 2).Discussion
mTBI often resulted in heterogeneous cognitive impairment as well as DTI metrics degenerating. However, these injures did not explain clinical outcome well. There were several subgroups with homogeneous features in the mTBI patients. Clustering is a widely used method which can figure out the number of subgroups among the patients, automatically. The result of clustering was highly consistent with that of the IPS, from which we can guess the determined 8 tracts may explain the outcome after suffering the brain injure. In addition, the clustering results in acute and 3-month period had a similar grouping situation, which meaned that the subgroups in the mTBI patients were relatively stable. But the variability of the grouping may indicate a more complex mechanism of mTBI injury. Besides, the first subgroup showed widespread white matter abnormalities compared with control individuals, while the second group only demonstrated circumscribed regional white matter abnormalities in the identified tracts.Conclusion
There were two main different subgroups in mild TBI patients and clustering is a reliable method to figure out the subgroups and to predict neuropsychological outcome among the mTBIs.Acknowledgements
This study was supported by the National Natural Science Foundation of China (Project Nos. 81371630, 81571752, the Shaanxi Nova program, the Fundamental Research Funds for the Central Universities, National key research and development plan of China, 2016YFC0100300.References
[1] M. E. Shenton, H M Hamoda, J S Schneiderman, et al. A review of magnetic resonance imaging and diffusion tensor imaging findings in mild traumatic brain injury. Brain Imaging and Behavior. 2012;(6):137-192.
[2] Smith, S.M., Jenkinson, M., Johansen-Berg, et al. Tractbased spatial statistics: voxelwise analysis of multi-subject diffusion data. NeuroImage. 2006;31:1487–1505.
[3] Huaiqiang Sun, Su Lui, et al. Two Patterns of White Matter Abnormalities in Medication-Naive Patients With First-Episode Schizophrenia Revealed by Diffusion Tensor Imaging and Cluster Analysis. JAMA Psychiatry. 2015; 72(7):678-86.
[4] Peter J.Hellyer, MRes,et al. Individual Prediction of White Matter Injury following Traumatic Brain Injury. Ann Neurol. 2013;73:489-499.
Figures