3334
Improved Reconstruction for Simultaneous Multi-Slice (SMS) Accelerated Interleaved EPI DWI1Center for Biomedical Imaging Research, Department of Biomedical Engineering, School of Medicine, Tsinghua University, Beijing, People's Republic of China, 2Vascular Imaging Laboratory, Department of Radiology, University of Washington, Seattle, WA, United States
Synopsis
Recently, simultaneous multi-slice (SMS) has been proved to be effective for accelerating single-shot EPI (ssh-EPI) based diffusion weighted imaging (DWI). More importantly, SMS can be combined with multi-shot interleaved EPI (iEPI) DWI to achieve high resolution and high throughput simultaneously. However, signal dropout problems may exist in the final DW images, especially at high SMS acceleration factors. The main reason is the prominent cerebrospinal fluid (CSF) pulsation, which may degrade the reconstruction performance. In this study, the reconstruction algorithm is augmented by using iteration and data rejection. In-vivo experiments have demonstrated that the augmented algorithm can effectively alleviate the signal dropout problems.
Purpose
Recently, simultaneous multi-slice (SMS) has been proved to be effective for accelerating single-shot EPI (ssh-EPI) based diffusion weighted imaging (DWI) (1,2). More importantly, SMS can be combined with multi-shot interleaved EPI (iEPI) DWI to achieve high resolution and high throughput simultaneously (3). However, signal dropout problems may exist in the inferior and medial regions of the brain, especially at high SMS acceleration factors. The reason is that the cerebrospinal fluid (CSF) pulsation in these regions is prominent, which may hamper the reconstruction of SMS accelerated iEPI DWI. In this study, the reconstruction algorithm is augmented by using iteration and data rejection. In-vivo experiments have demonstrated that the augmented algorithm can effectively alleviate the signal dropout problems.Methods
Experiments All scans were performed on a Philips 3.0T Achieva TX MRI scanner (Philips Healthcare, Best, The Netherlands) using a 32-channel head coil. All human studies were performed under IRB approval from our institution. For the SMS acquisitions, traditional 90° excitation and 180° refocusing RF pulses were frequency modulated and summed. An 8-shot iEPI DWI acquisition with SMS acceleration factor MB=3 was performed with gap=44 mm and FOV/3 shift. The sequence diagram was the same as described in ref. (3), with an SMS 3D navigator to record the inter-shot phase variations. Other imaging parameters were: FOV=216×216×132 mm3 (sagittal orientation), voxel size=1×1×4 mm3, TE=72 ms, TR=3.6 s, partial Fourier=0.7. Diffusion encoding was applied in 3 orthogonal directions with b=800 s/mm2. Meanwhile, an 8-shot iEPI acquisition without SMS acceleration were also performed as references, with other imaging parameters kept the same.
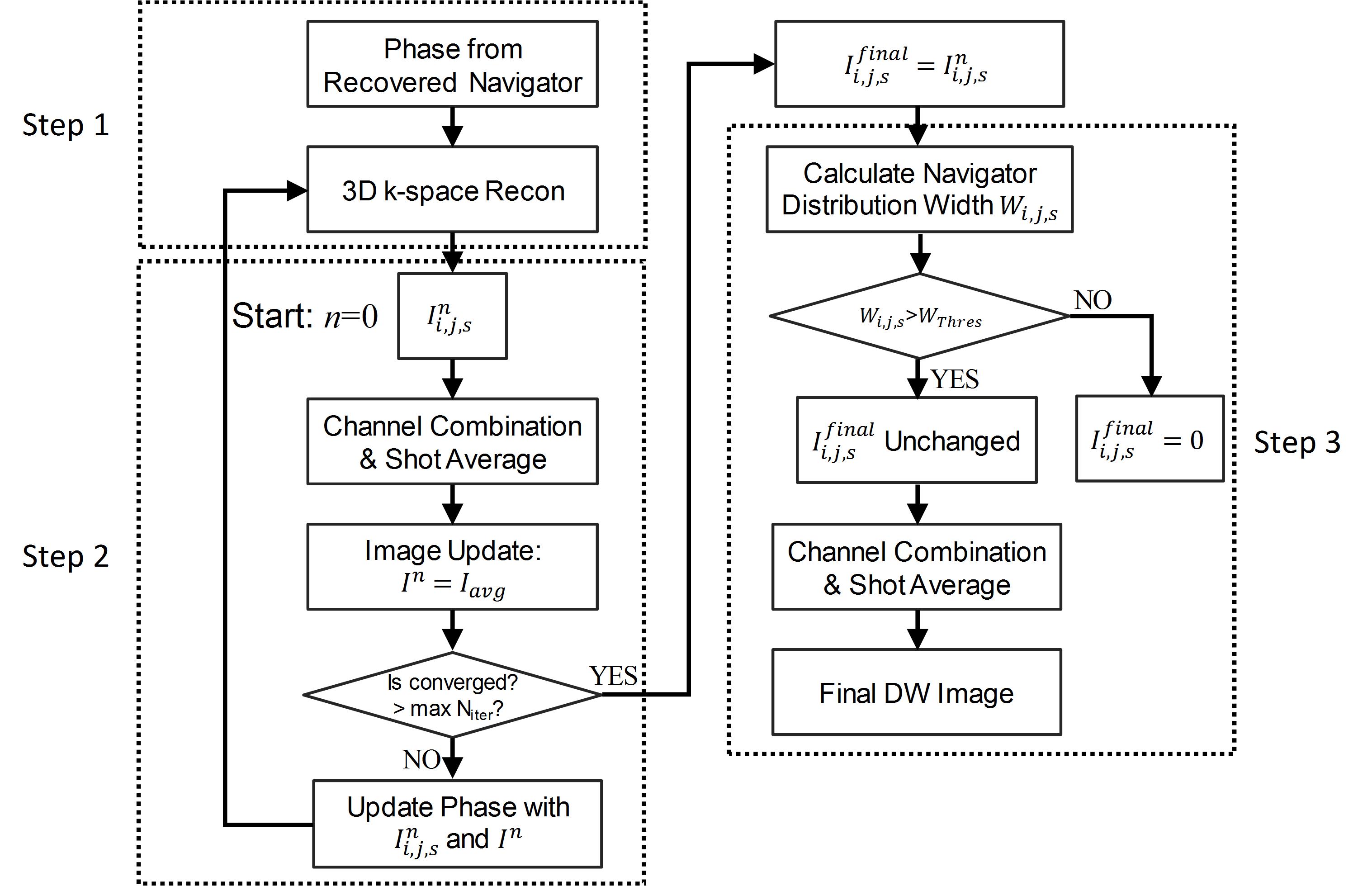
Reconstruction The flowchart of the augmented 3D k-space reconstruction with iteration and data rejection is shown in Fig. 1.
Step 1: The initial 3D k-space reconstruction. As described in ref. (3), the under-sampled SMS 3D navigator is first recovered to calculate the phase variations. Then the SMS 3D k-space reconstruction (3) is performed to recover the image $$$I_{i,j,s}^{0}$$$, where $$${i,j,s}$$$ is the index for shot, channel and slice, respectively.
Step 2: The iterative reconstruction. The iteration process is similar to ref. (4), including:
2.1) $$$I_{i,j,s}^{n}$$$ from different channels and shots are combined to generate an average image $$$I_{avg}$$$. The initial result from step 1 is used as $$$I_{i,j,s}^{0}$$$.
2.2) The image estimation is updated by $$$I^{n}=I_{avg}$$$.
2.3) If the difference between $$$I^{n}$$$ and $$$I^{n-1}$$$ is smaller than a predefined tolerance τ or the iteration number exceeds the predefined maximum iteration number $$$N_{iter}$$$, the iteration ends and $$$I_{i,j,s}^{n}$$$ is selected as the final result. Otherwise, the inter-shot phase estimation for each shot is updated with $$$I_{i,j,s}^{n}$$$ and $$$I^{n}$$$, which will be used in next iteration.
Step 3: The data rejection step. Previous study has shown that the distribution width of the navigator can be used to detect the severely corrupted data (5). The distribution width $$$W_{i,j,s}$$$ of the recovered navigator from each shot and each slice is first calculated. If $$$W_{i,j,s}$$$ is larger than a predefined threshold (1.05 in this study), $$$I_{i,j,s}$$$ is excluded from the calculation of the final DW image.
It should be noted that step 2 and 3 can be used independently or together. Once the final DW images are obtained, ADC maps are calculated and compared with the un-accelerated 8-shot iEPI DWI results.
Results and Discussion
Fig. 2 shows the DW image (from one diffusion encoding direction) comparison among different reconstruction. Only one slice is shown for space consideration. As shown, when the SMS 3D k-space reconstruction incorporates iteration and/or data rejection, the signal dropouts in the central regions of the brain can be well recovered (yellow arrowheads). The corresponding ADC maps are shown in Fig. 3, with the one without SMS acceleration as a reference. For better illustration, the ADC differences between the SMS accelerated acquisition (MB=3) and un-accelerated acquisition (MB=1) are also shown. Using the original 3D k-space reconstruction, the signal dropouts in the central of the brain can cause higher ADC values than the reference. The ADC maps with iteration and/or data rejection are closer to the un-accelerated result. However, there are still some residual errors (red arrowheads) for the reconstruction if using data rejection only.Conclusion
In this study, the original 3D k-space reconstruction for SMS accelerated iEPI DWI has been optimized using iteration and data rejection. In-vivo experiments have demonstrated that the augmented algorithm can effectively alleviate the signal dropout problem and improve the precision of quantitative calculation, such as ADC maps. The improved reconstruction is beneficial for applying high resolution iEPI DWI to clinical diagnosis and neuroscience studies.Acknowledgements
No acknowledgement found.References
1. Setsompop K, Cohen-Adad J, Gagoski BA, Raij T, Yendiki A, Keil B, Wedeen VJ, Wald LL. Improving diffusion MRI using simultaneous multi-slice echo planar imaging. Neuroimage 2012;63:569-580.
2. Feinberg DA, Moeller S, Smith SM, Auerbach E, Ramanna S, Glasser MF, Miller KL, Ugurbil K, Yacoub E. Multiplexed echo planar imaging for sub-second whole brain FMRI and fast diffusion imaging. PLoS One 2010;5e15710.
3. Dai E, Ma X, Zhang Z, Yuan C, Guo H. Simultaneous multislice accelerated interleaved EPI DWI using generalized blipped-CAIPI acquisition and 3D K-space reconstruction. Magn Reson Med 2016; DOI: 10.1002/mrm.26249.
4. Guo H, Ma X, Zhang Z, Zhang B, Yuan C, Huang F. POCS-enhanced inherent correction of motion-induced phase errors (POCS-ICE) for high-resolution multishot diffusion MRI. Magn Reson Med 2016;75:169-180.
5. Porter DA, Heidemann RM. High resolution diffusion-weighted imaging using readout-segmented echo-planar imaging, parallel imaging and a two-dimensional navigator-based reacquisition. Magn Reson Med 2009;62:468-475.
Figures