3307
Respiratory motion-resolved MRI of the lung and liver for evaluation of cystic fibrosis1Brain Institute of Rio Grande do Sul (Brains) - PUCRS, Porto Alegre, RS, Brazil, 2Graduate Program in Pediatrics and Child Health PUCRS, Porto Alegre, RS, Brazil, 3Graduate Program in Electrical Engineering PUCRS, Porto Alegre, RS, Brazil, 4Graduate Program in Medicine and Health Sciences PUCRS, Porto Alegre, RS, Brazil, 5Center for Advanced Imaging Innovation and Research New York University School of Medicine, New York, NY, United States
Synopsis
Free-breathing MRI with reconstruction of respiratory phases using the XD-GRASP technique is demonstrated for evaluation of cystic fibrosis patients. A platform for automated data processing is developed for robust utilization in a clinical setting. XD-GRASP is validated in a cohort of 9 patients against the conventional technique.
Purpose
Cystic fibrosis requires high resolution volumetric imaging of the lungs and liver (1). The current standard technique is CT (2), which can potentially expose to patients to cumulative high radiation doses. MRI has become a radiation-free alternative to CT (3). However, despite the significant progress in terms of speed and motion navigators, MRI is still sensitive to respiratory motion, which limits the achievable volumetric coverage and spatial resolution. XD-GRASP (4) is a recent addition to the large set of free-breathing MRI technique that might be a game changer for imaging during respiratory motion. Instead of correcting or gating motion, XD-GRASP reconstructs an additional dimension with respiratory phases, by exploiting the data sorting properties of golden-angle radial imaging and the compressibility of respiratory motion. In this work, we demonstrate the application of XD-GRASP lung and liver MRI for evaluation of cystic fibrosis patients. A whole pipeline for automated data processing is developed for robust utilization in a clinical setting. Free-breathing XD-GRASP is validated against the current 3D MRI technique with breath-hold in a cohort of 9 patients.Methods
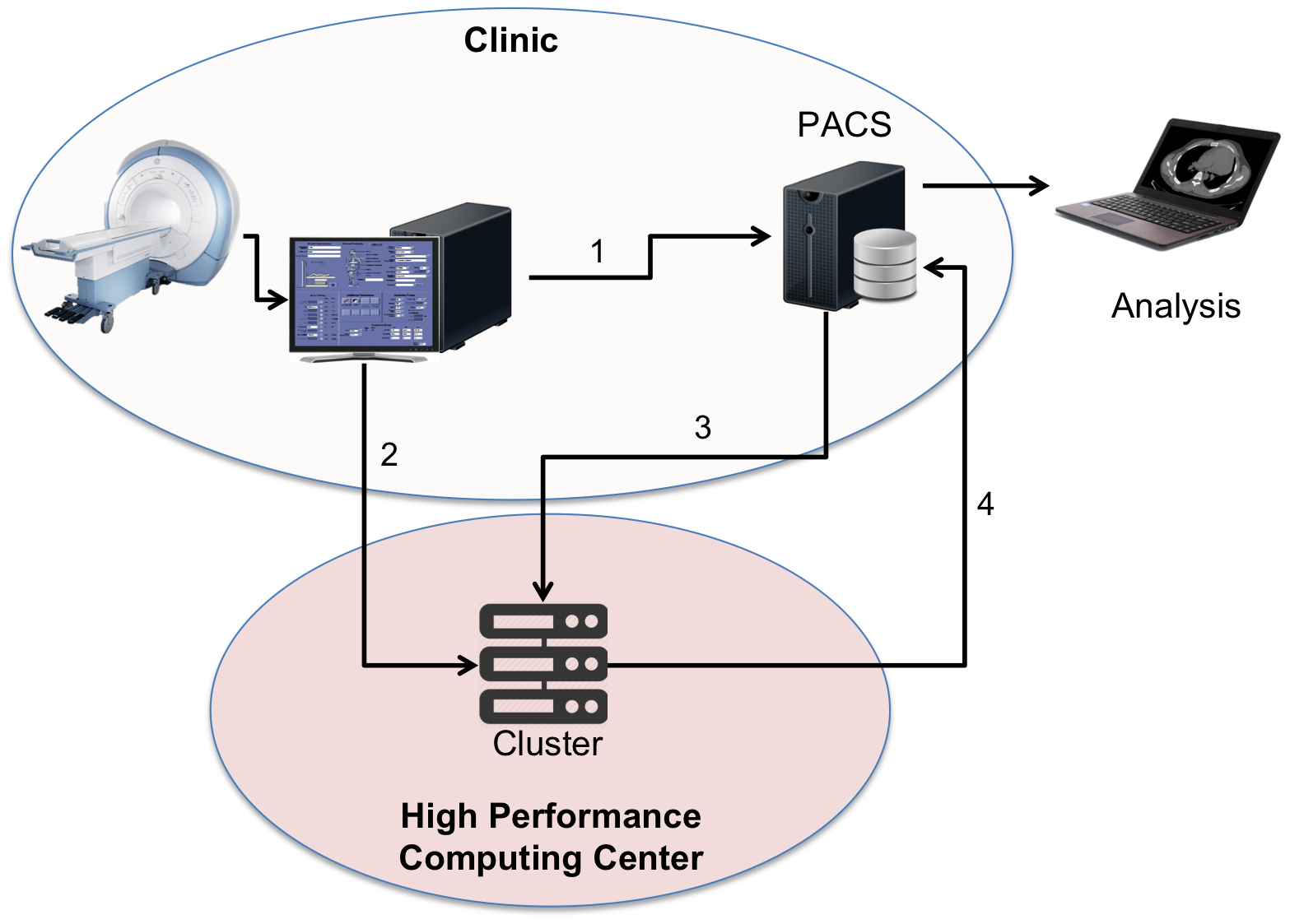
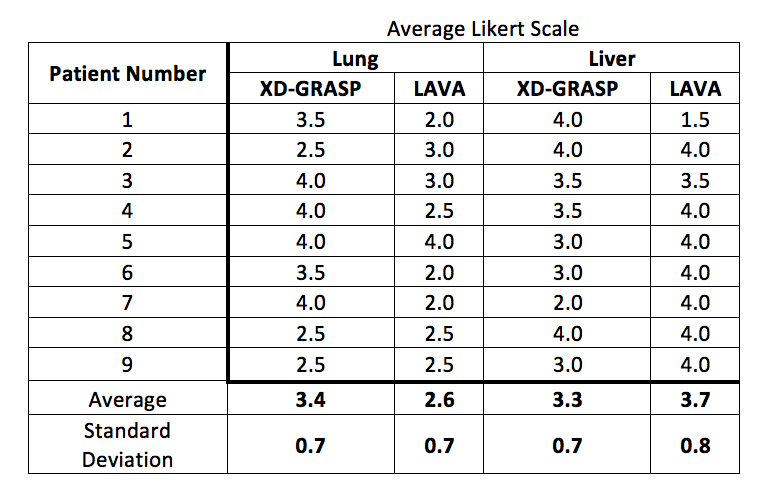
XD-GRASP: A T1-weighted 3D pulse sequence with golden-angle stack-of-stars sampling was developed to perform free-breathing continuous imaging in the lung and liver. In order to reduce sensitivity to respiratory motion along the Cartesian kz dimension, all kz points were acquired for each radial angle before encoding the next one. Respiratory motion signal was estimated directly from the data by collecting the central k-space points for each angle into the columns of a kz-angle matrix and applying Principal Component Analysis (4). The continuously acquired data were sorted into different respiratory states, which formed an additional 4th dimension. Compressed sensing reconstruction was performed on the sorted undersampled dataset by enforcing sparsity in the difference between adjacent respiratory states (minimization of total variation along the respiratory motion dimension). Automated data processing (Figure 1): In order to facilitate the utilization of XD-GRASP in a clinical setting, we have developed a complete data processing pipeline from raw data reading to reconstruction results in the clinical database (PACS). Once the MRI scan has finalized, the raw data file is automatically transferred to a high-performance computer to be reconstructed using the XD-GRASP algorithm. Finally, reconstruction results in dicom format are transferred to the PACS server for clinical evaluation. Clinical MRI studies: Lung and liver data were acquired on 9 patients referred for evaluation of cystic fibrosis using conventional breath-held LAVA and XD-GRASP on a 3.0T scanner (Signa HDxt, GE Heathcare). Relevant imaging parameters for LAVA include: TR/TE= 3.9/1.8 ms, flip angle= 10o, FOV= 400x400mm2, in-plane image matrix= 512x512, slices= 92, slice thickness= 2.0mm, data acquisition time = 19 seconds. Imaging parameters for XD-GRASP include: TR/TE= 12.7/2.6 ms, flip angle= 10o, FOV= 440x440 mm2, in-plane image matrix= 352x382, slices= 40, slice thickness= 4.0mm, data acquisition time = 96 seconds. XD-GRASP images were reconstructed with 4 respiratory phases. For lung studies, the inspiration and expiration phases were employed. For liver studies, the end-expiration phase was used. Image quality assessment: Conventional-LAVA and XD-GRASP results were anonymized and presented to two expert radiologists in a random fashion for blinded evaluation. Image quality was scored using a using a Likert scale (1-unacceptable to 5-outstanding). Wilcoxon signed-rank tests were performed to statistically compare image quality.Results
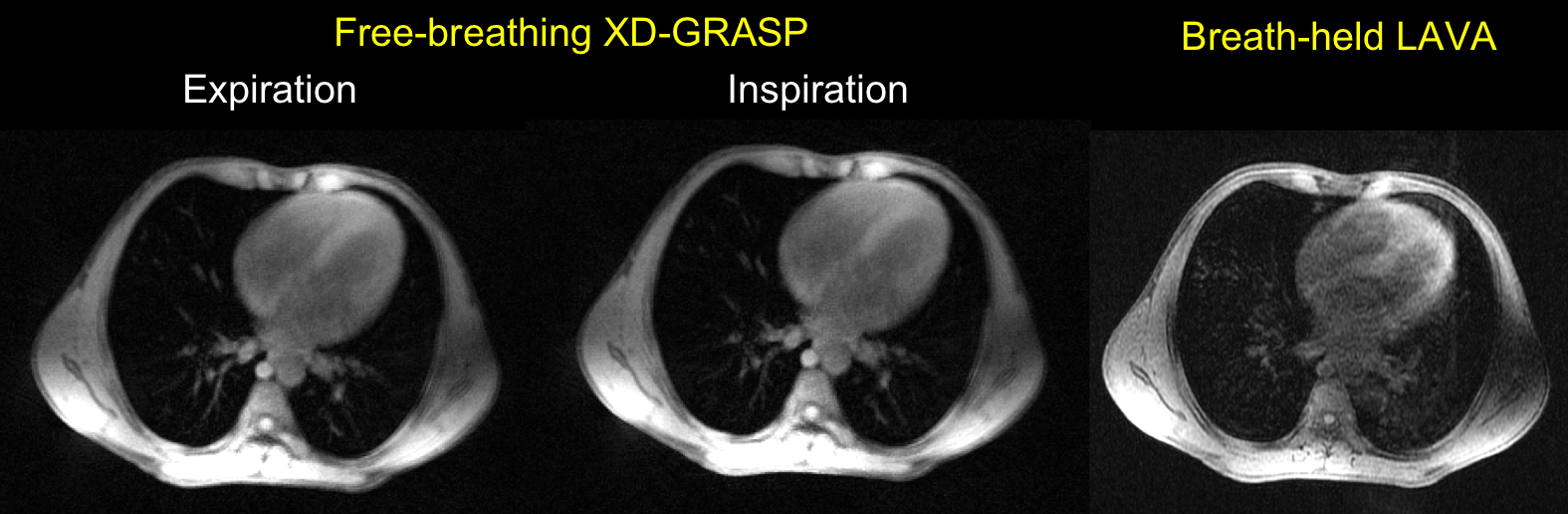
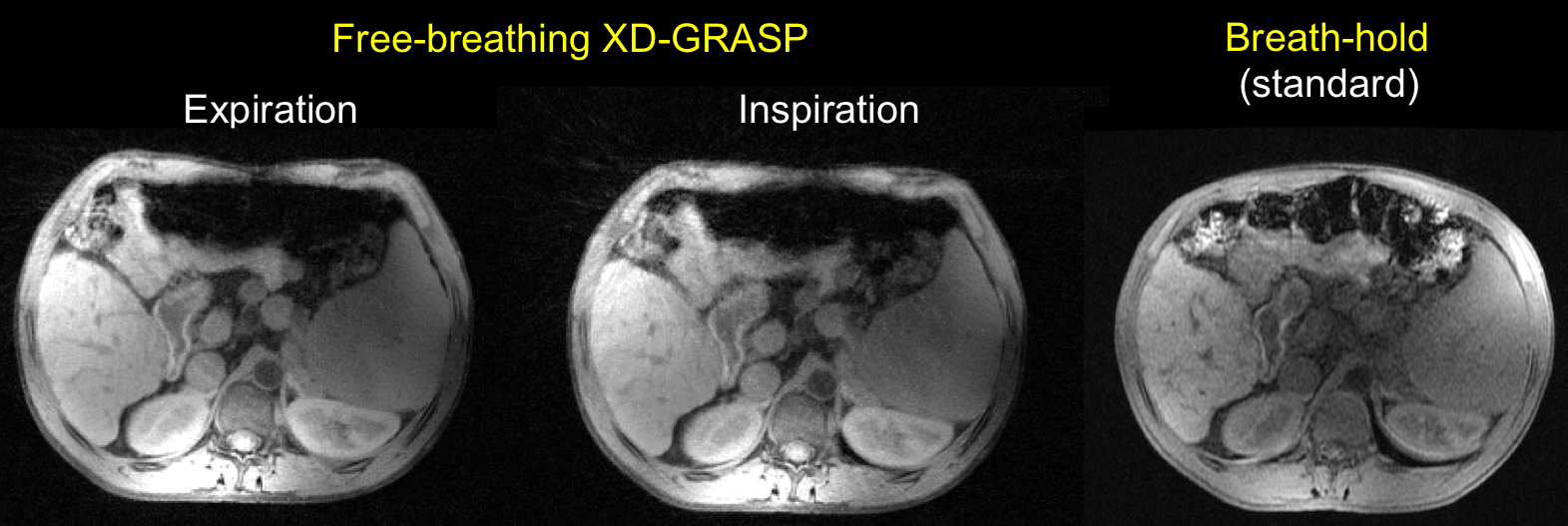
The higher motion robustness of XD-GRASP resulted in improved image quality with respect to conventional breath-held LAVA in the lungs and liver (Figures 2-3). In particular lung images were significantly improved as they are more affected by respiratory motion (Figure 2). Both readers agreed on significant improvement in the lungs and similar performance in the liver (Figure 4). The results in the lungs were also found to be statistically significant (p<0.05).Discussion
XD-GRASP overcomes the major limitation of MRI for evaluation of cystic fibrosis, this is, artifacts produced by respiratory motion, especially in lung examinations. Moreover, access to information from different respiratory phases enable to compute air traps in a similar fashion to CT but without exposure to radiation. The addition of these two points promises to improve diagnostic accuracy, as it was shown in this cohort of patients. The automated data processing pipeline represents an important tool for clinical translation and may be used for different applications.Conclusion
We have demonstrated the application of XD-GRASP for free-breathing MRI of the lungs and liver for evaluation of cystic fibrosis patients using a fully-automated data processing pipeline. This development may help to increase the use of MRI in this patient population.Acknowledgements
We would like to thank technoligists at InsCer for data collection, patients for their collaboration, and CAPES (88881.030420/2013-01) for financial support.References
1 - Davis PB, Drumm M, Konstan MW. Cystic fibrosis. Am J Respir Crit Care Med. 1996;154(5):1229-56.
2- Davis SD, Fordham LA, Brody AS, et al. Computed tomography reflects lower airway inflammation and tracks changes in early cystic fibrosis. Am J Respir Crit Care Med 2007; 175: 943–950.
3- Carr DH, Oades P, Trotman-Dickenson B, et al. Magnetic resonance scanning in cystic fibrosis: comparison with computed tomography. Clin Radiol 1995; 50: 84–89.
4-Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn Reson Med. 2016 Feb;75(2):775-88.
Figures