3296
Free breathing prospectively navigated renal BOLD for improved SNR and T2* accuracyGlen Morrell1 and Vivian S. Lee1
1Radiology and Imaging Sciences, University of Utah, Salt Lake City, UT, United States
Synopsis
A prospectively gated free-breathing renal BOLD sequence was compared to conventional breath hold renal BOLD. The new sequence gives consistently better SNR than the conventional sequence. RMS error of T2* estimation was investigated as a measure of accuracy. The free-breathing renal BOLD sequence allows flexible tradeoff of imaging time with SNR and can improve the accuracy of renal BOLD T2* estimation.
Purpose
To evaluate the accuracy of a novel free-breathing prospectively navigated method of renal BOLD compared to conventional breath-hold renal BOLD.Introduction
Renal BOLD MRI shows promise for the evaluation of oxygen levels in the kidneys. Hypoxia is thought to play a central role in the development and progression of chronic kidney disease. A noninvasive method for measuring renal oxygen levels would have great scientific and clinical impact. Renal BOLD results have been exciting but contradictory, possibly because of limitations of the underlying MRI methods. The kidneys move with respiration, limiting human renal BOLD to a single breath hold with limited SNR, resolution, and coverage. Methods are needed to break the breath hold barrier to allow a flexible tradeoff between imaging time and SNR and resolution. We recently introduced a free-breathing prospectively gated renal BOLD sequence (FB-BOLD) which can extend imaging time beyond a single breath hold (1). In the current work we evaluate this method compared to conventional breath hold renal BOLD (BH-BOLD) for the case of single slice 2D renal BOLD.Methods
The FB-BOLD sequence is illustrated in Figure 1. The sequence runs with constant repetition time. A slice-selective navigator is acquired at the beginning of each sequence repetition and analyzed in real time to bin the image data based on the phase of the respiratory cycle, with feedback to the running sequence to acquire the appropriate next phase encoding step. When one bin contains a complete k-space the sequence is finished. The resulting BOLD source images are free of respiratory motion artifact. Since data acquisition takes place during free breathing, there is no constraint on total image time. For 2D single-slice renal BOLD MRI, this freedom can be used to acquire multiple signal averages, thus increasing SNR. We recruited 10 healthy volunteers for this IRB-approved HIPAA-compliant study. Each subject underwent conventional BH-BOLD with a single coronal image obtained through the largest cross-section of the kidneys, and FB-BOLD with identical sequence parameters but longer imaging time to allow four signal averages. Sequence parameters for this study included GRE acquisition, matrix size 256x256 over a 360x360mm FOV, 8mm slice thickness, 300 Hz pixel bandwidth, TE=(5,10,15,20,25,30,35,40)msec, FA=25, fat saturation, and 1 signal average for breath hold and 4 for FB-BOLD. BH-BOLD TR was 58 msec while the FB-BOLD TR was 95 msec, reflecting the extra time necessary for navigation and real-time sequence feedback. Total BH-BOLD imaging time was 15 sec compared to about 3:00 minutes for FB-BOLD. Efficiency of the FB-BOLD sequence is about 50-60% (i.e. 50-60% of the collected data is used in the final images). Image data was analyzed by manual segmentation of right and left kidney. SNR and mean squared error of T2* fitting were quantified for right and left kidney separately.Results
Figure 3 compares SNR between the BH-BOLD and FB-BOLD sequences. The FB-BOLD sequence gives consistently higher SNR by an average factor of 1.87 for the right kidney and 1.94 for the left kidney. Figure 4 shows the RMS error of T2* estimation averaged over the kidney. T2* estimation error for FB-BOLD is 0.65 that of BH-BOLD for the right kidney, 1.25 for the left kidney.Discussion
The FB-BOLD sequence shows expected increase in SNR made possible by breaking the breath hold barrier with free breathing acquisition. Increased SNR is expected to result in more accurate T2* estimation. Interestingly, the RMS error of T2* estimation is lower in the right kidney with the FB-BOLD sequence but increased in the left kidney. This error gives some indication of the accuracy of T2* estimation but must be interpreted with caution, since local B0 inhomogeneity can cause the actual signal decay to deviate significantly from an ideal exponential (2). The difference between right and left kidney likely reflects the placement of the navigator plane across the right kidney and diaphragm.Conclusion
The free-breathing prospectively navigated renal BOLD sequence achieves expected improvements in SNR compared to a conventional breath hold renal BOLD sequence. Navigation improves the accuracy of T2* estimation of the kidney nearest the navigator but may not improve T2* estimation of the contralateral kidney.Acknowledgements
This work was supported by NIH/NIDDK grant R01 DK063183References
1. Morrell G et al.: Prospectively navigated multi-echo GRE sequence for improved 2D BOLD imaging of the kidneys. 21st Meeting ISMRM. Salt Lake City, 2013 pp 1569.
2. Hernando D et al.: R*(2) mapping in the presence of macroscopic B(0) field variations. Magn Reson Med, 68: 830-840, 2012.
Figures
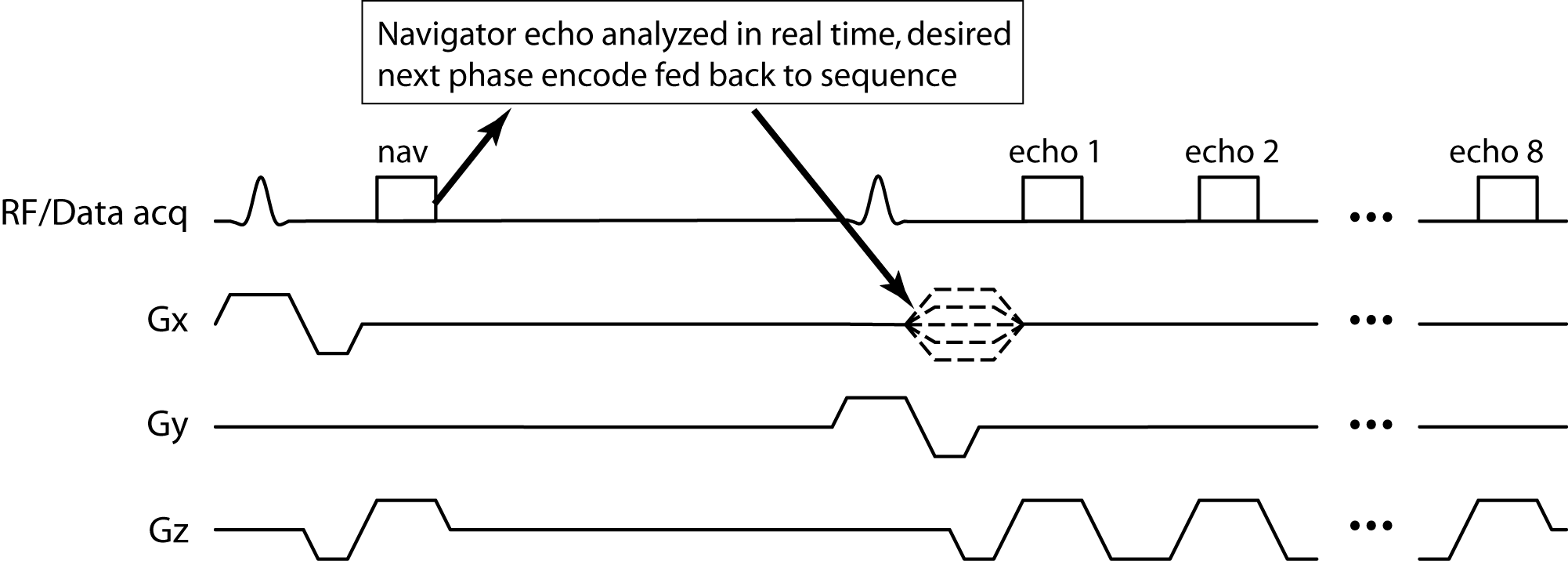
Figure 1: Pulse sequence diagram of the FB-BOLD sequence. The sequence runs
at constant TR and acquires a navigator at the beginning of each repetition, typically
placed across the right diaphragm. The navigator is processed in
real-time and feedback is provided to the running sequence to specify the phase
encoding step to be acquired.
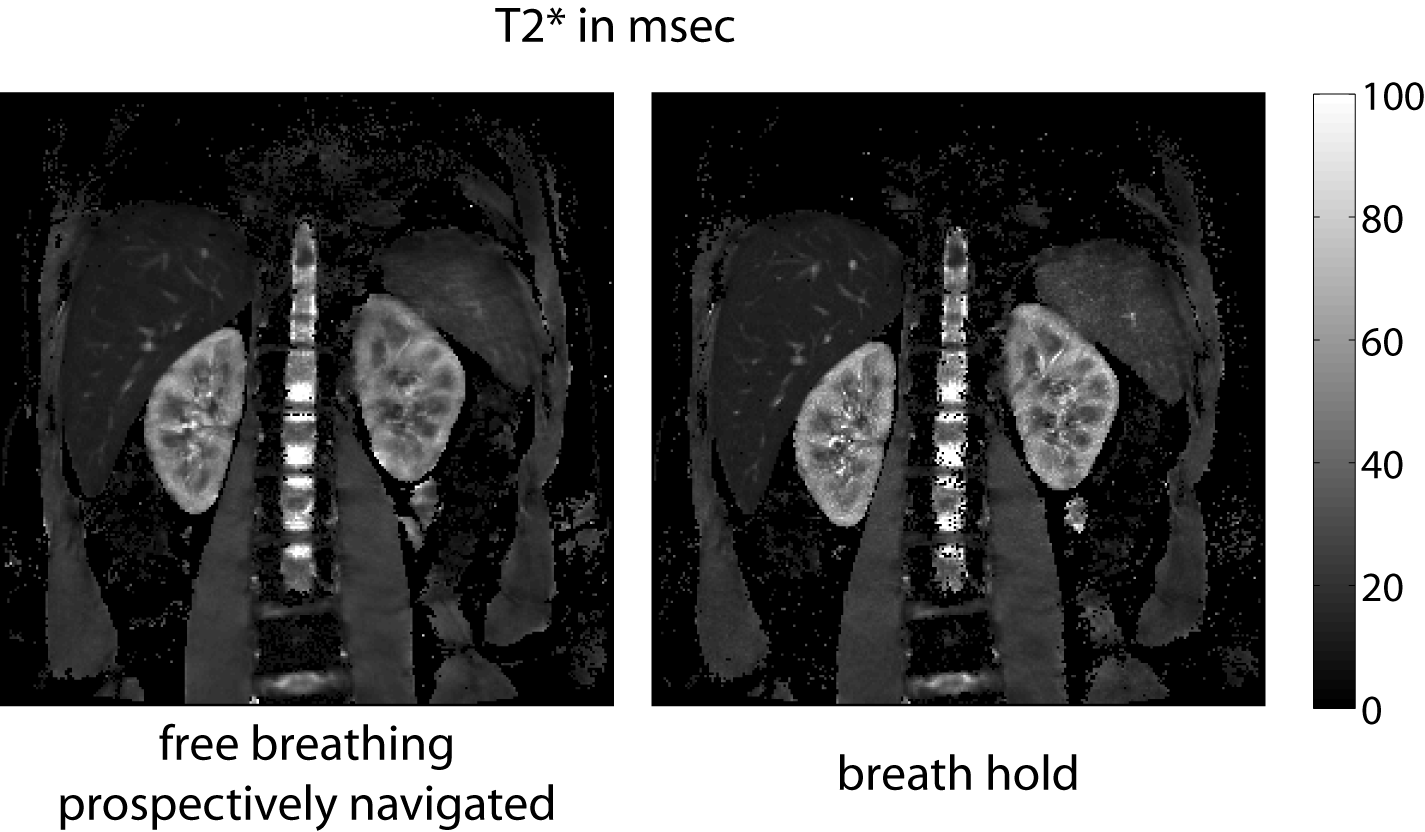
Figure 2: Example of T2* maps with conventional
breath hold sequence (BH-BOLD) and prospectively navigated free-breathing
sequence (FB-BOLD).
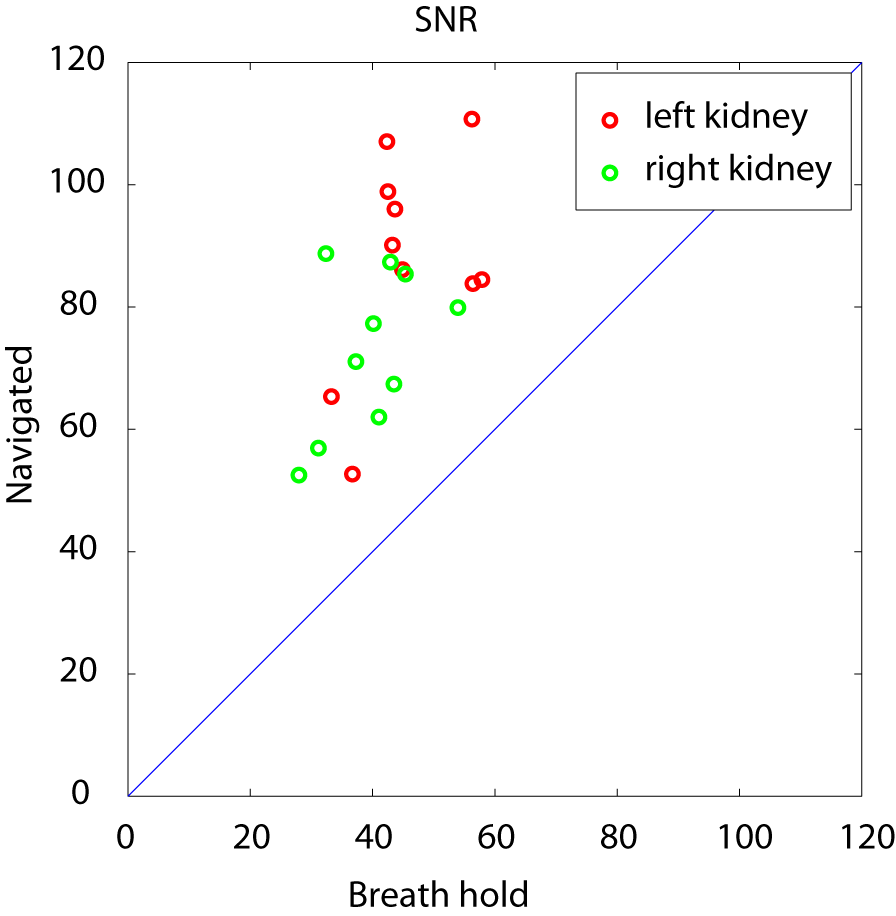
Figure 3: SNR comparison of FB-BOLD and BH-BOLD. The
prospectively navigated free-breathing sequence consistently achieves increased
SNR in both right and left kidneys.
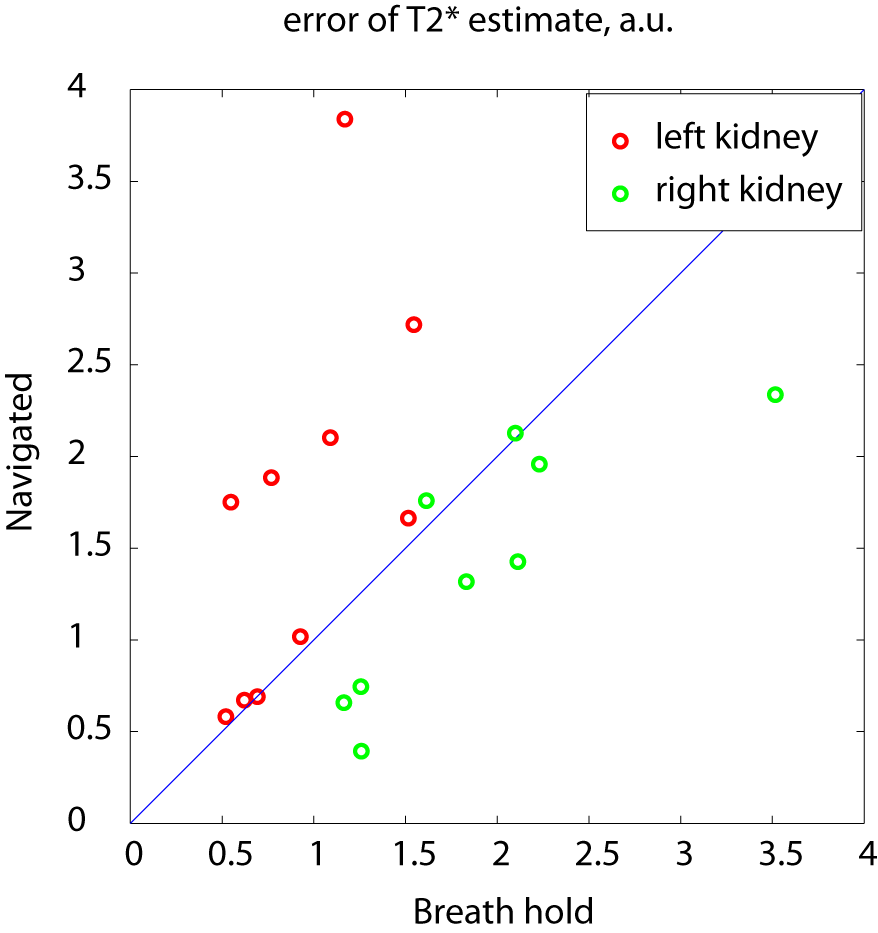
Figure 4: Comparison of root mean squared error of T2*
estimation. One outlier in which navigation failed is excluded from this
plot. The FB-BOLD sequence gives lower RMS T2* estimation error in the
right kidney, but increased error in the left kidney compared to BH-BOLD.
This is likely related to placement of the navigator over the right kidney and
diaphragm and suggests that navigator placement may be important for the
FB-BOLD sequence.