3281
Vascular Access Mapping with Ferumoxytol MRA for TAVR Planning in Patients with Renal Impairment: A Step Closer Towards Patient-Specific Care1Diagnostic Cardiovascular Imaging Laboratory, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 2Division of Cardiology, David Geffen School of Medicine at UCLA and VA Greater Los Angeles Healthcare System, 3Department of Radiological Sciences, David Geffen School of Medicine at UCLA
Synopsis
Transcatheter aortic valve replacement (TAVR) has transformed the treatment of critical aortic stenosis, particularly for those patients whose surgical operative risks are high. However, pre-TAVR vascular mapping with CT requires 40-120 mls of iodinated contrast, which in older patients with renal impairment increases the risk of acute renal injury that portends poor prognosis. We demonstrated that ferumoxytol MRA can provide reliable vascular mapping in patients with renal impairment undergoing TAVR evaluation, without exposure to iodinated or gadolinium contrast agents.
PURPOSE
Advances in transcatheter aortic valve replacement (TAVR) have increasingly enabled an older population to undergo aortic valve replacement for severe aortic stenosis, particularly in cases where surgical operative risks would be moderate or high. However, renal impairment is a major hurdle in older patients who require pre-TAVR vascular mapping for procedural planning. Poor baseline renal function as well as acute renal failure at the time of TAVR has been shown to portend worse mortality and morbidity (1). Investigators have recently explored the off-label use of ferumoxytol (FE) as a blood pool MRA contrast agent (2), whereas its FDA-approved therapeutic use is for treatment of anemia in patients with renal failure. We aim to assess the diagnostic performance of ferumoxytol MRA for pre-TAVR vascular access mapping in patients with renal impairment.METHODS
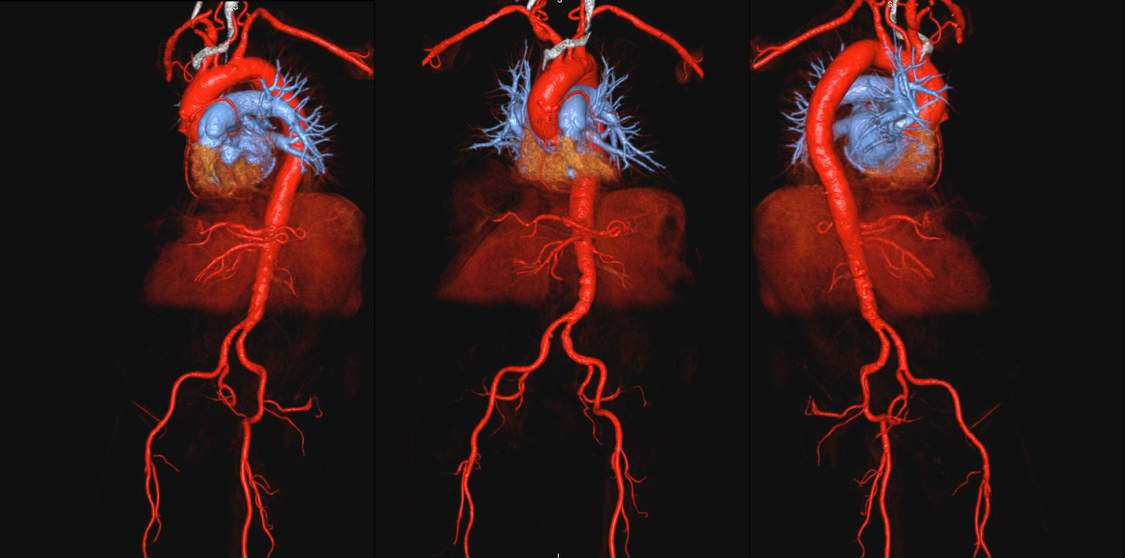
After written informed consent, FE-MRA was performed at 3.0T (n=23) or 1.5T (n=3) with an infusion of ferumoxytol up to 4mg/kg. Patients with cardiac devices (n=3) were studied at 1.5T. Multi-station, high resolution 3D MRA datasets were acquired with overlap and composed to a single extended field of view 3D set. To assess the vascular calcification burden, non-contrast CT images were registered and fused to FE-MRA images. Image quality of the aorto-iliofemoral arterial tree (n=8 segments per patient) was evaluated with respect to calcific burden, vessel tortuosity, and luminal diameter using a 4-point scale with a score of 4 representing excellent vascular definition such that detailed anatomy is clearly visualized with sharp borders.RESULTS
Of 285 unique patients undergoing FE-MRI for clinical indication at our institution, twenty-six patients (ages 82±11 years, 9 females) underwent institution-specific FE-MRA pre-TAVR vascular mapping protocol. The average estimated glomerular filtration rate at the time of FE-MRI was 32±11 mL/min/1.73m2 (creatinine 2.1±0.8 mg/dL). Pre- and post-TAVR hemoglobin were 11.3±2.3 and 10.2±1.9 g/dL, respectively. All patients underwent FE-MRI safely and without adverse events. A total of 200 vascular segments were evaluated. The average image quality score was 4 for all segments evaluated. There was perfect inter-observer agreement (k=1). In 21 patients with fused non-contrast CT and FE-MRA images, fusion allowed readers to qualitatively assess vascular calcific burden and location along the course of the vessels. Of the 26 patients who had FE-MRA, three patients had surgical AVR, three died prior to TAVR, and one case was aborted. Of those that underwent TAVR (n=19), thirteen patients had trans-femoral and six had trans-apical access. At an average follow-up time of 1.9±0.5 years, four of the 19 patients died from coexisting medical conditions. One patient required duplex ultrasound to confirm the small vessels depicted on FE-MRA. In all cases, there were no peri-operative vascular complications.CONCLUSION
In patients with renal impairment undergoing TAVR, a patient-specific protocol with ferumoxytol MRA provides reliable vascular mapping without exposure to iodinated or gadolinium contrast agents. Thus, the total cumulative dose of iodinated contrast is minimized and the risk of acute nephropathy is reduced.Acknowledgements
No acknowledgement found.References
1. Sinning JM et al. Renal function as predictor of mortality in patients after percutaneous transcatheter aortic valve implantation. JACC Cardiovasc Interv. 2010;3:1141–1149.
2. Finn JP et al. Cardiovascular MRI with ferumoxytol. Clinical Radiology. 2016 Aug;71(8):796-806.
Figures