3279
4D Ferumoxytol Enhanced MUSIC: Value-Based MRI in Neonates and Infants with Congenital Heart Disease1Diagnostic Cardiovascular Imaging Laboratory, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 2Division of Cardiology, David Geffen School of Medicine at UCLA and VA Greater Los Angeles Healthcare System, 3Department of Radiological Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 4Department of Anesthesiology, David Geffen School of Medicine at UCLA, 5Division of Pediatric Cardiology, David Geffen School of Medicine at UCLA, 6Department of Cardiothoracic Surgery, David Geffen School of Medicine at UCLA
Synopsis
Conventional cardiovascular magnetic resonance imaging (MRI) in congenital heart disease (CHD) enables dynamic morphologic and vascular assessment. However, current techniques require multi-slice cine imaging and angiography with supplemental phase-contrast. We demonstrate that 4D multiphase steady state imaging with contrast (MUSIC) can provide high-resolution dynamic images of all relevant cardiovascular anatomy without breath-holding or operator input in a cohort of neonates and infants with CHD. Further, 4D MUSIC has high clinical impact on the care of small children.
PURPOSE
MRI plays a vital role in congenital heart disease (CHD) imaging without ionizing radiation. Conventional CHD MRI exams require multi-slice cine acquisition, angiography, and phase-contrast imaging. Recently, a 4D (MUSIC) technique has been described1,2, which generates high-resolution 3D dynamic images of the beating heart during uninterrupted ventilation. We evaluated the diagnostic performance and clinical impact of 4D MUSIC in neonates and infants with congenital heart disease (CHD).METHODS
Forty consecutive children with CHD (age range 2 days to 2 years, weight 1 to 13 kg) underwent MRI with ferumoxytol (FE) at 3.0T and were prospectively enrolled. Two readers graded the diagnostic image quality of intra-cardiac structures and vascular segments including coronaries using a four-point scale. A score of 4 reflects excellent image quality with well-defined, sharp borders whereas a score of 1 reflects non-diagnostic image quality. Correlation of FE-MUSIC findings with other imaging modalities and/or surgical reports was performed. Clinical impact was assessed on a five-point scale (one point per key measure): 1) change in overall management, 2) change in surgical approach, 3) elimination of need for diagnostic catheterization, 4) improved assessment of risk-to-benefit for planned intervention and discussion with parents, and 5) accurate pre-procedural roadmapRESULTS
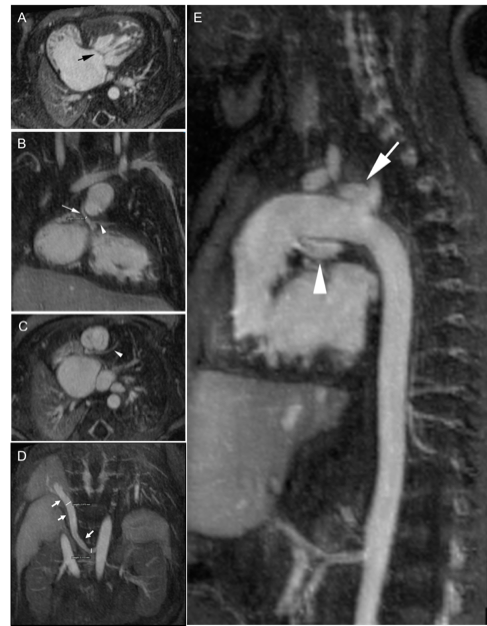
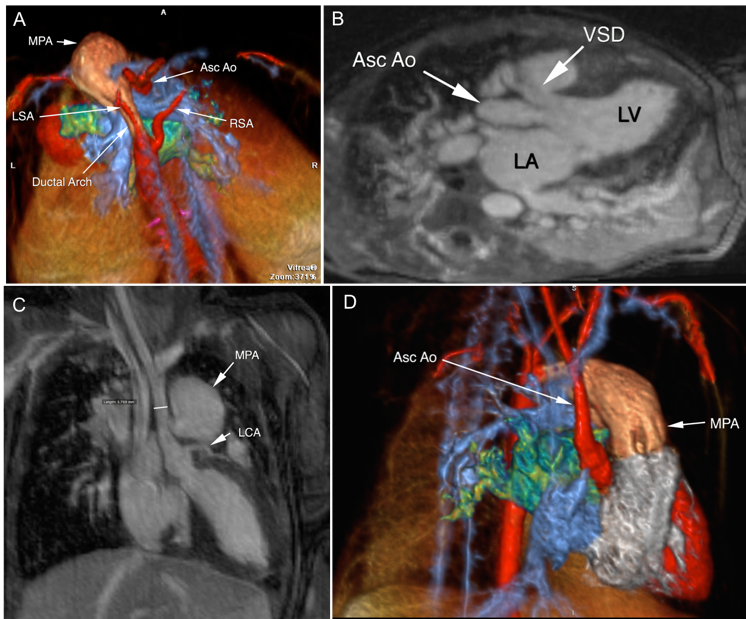
All studies were technically successful and there were no adverse events. In all cases, FE-MUSIC satisfactorily answered all clinical questions requested by referring surgeons or cardiologists and in many cases provided additional insight, which impacted the overall patient care plan. On a four-point scale, the average FE-MUSIC image quality scores were >3.5 for intra-cardiac structures and >3.0 for coronary arteries. Intra-cardiac morphology and vascular anatomy were visualized with good interobserver agreement (r=0.46). Tiny structures such as the course of a 1mm vestigial aortic root in a neonate weighing 3.6 kg was well-visualized (Figure 1). Concordance with correlative imaging, surgical, and /or autopsy results was excellent. In five patients with discordant findings on echo /MUSIC (n=5) and catheter angiography /MUSIC (n=1), findings on FE-MUSIC were shown to be accurate at autopsy (n=1) and surgery (n = 4). The clinical impact score was 4.2±0.9. Surgical management was affected in all cases. Of the 28 cases where management may have called for cardiac catheterization to assess vascular anatomy, diagnostic cath was avoided in 13 patients because vascular anatomy and its relationship to intracardiac morphology were well visualized on FE-MUSIC imaging (Figure 2). In 75% of cases, clinical impact was affected across more than four key outcome measures.CONCLUSION
FE-MUSIC provides reliable high-resolution dynamic imaging of all relevant cardiac and vascular anatomy in neonates with CHD. By obviating the need for breath holding and operator input, FE-MUSIC promises to enhance the practicality and generalizability of MRI in children.Acknowledgements
This work is supported by grant R01HL127153 from the National Heart, Lung, and Blood Institute.References
1. Fei Han, et al. 4-Dimensional, Multiphase, Steady-state Imaging with Contrast Enhancement (MUSIC) in the Heart; a Feasibility Study in Children. Mag Reson Med 2015 Oct;74(4):1042-9.
2. Fei Han, et al. Self-gated 4D Multiphase, Steady-state Imaging with Contrast Enhancement (MUSIC) using Rotating Cartesian K-space (ROCK): Validation in Children with Congenital Heart Disease. Magn Reson Med. 2016 Aug 16. Epub ahead of print.
Figures