3276
Cardiac Cine MRI with bSSFP-EPI at 0.35T1Radiological Sciences, University of California, Los Angeles, Los Angeles, CA, United States, 2Radiation Oncology, University of California, Los Angeles, Los Angeles, CA, United States, 3Biomedical Physics Graduate Program, University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
We have developed a bSSFP-EPI cine sequence and implemented it on a 0.35T MR system. The bSSFP-EPI cine sequence has reduced acquisition duration compared to conventional bSSFP cine.
Purpose
Balanced steady state free precession (bSSFP) is considered the workhorse for cardiac cine MRI owing to its superior contrast between blood and myocardium1. Our institution recently installed a real time MRI-guided radiotherapy system (ViewRay Inc., Oakwood Village, OH), which includes a 0.35T superconducting MRI system and a Cobalt-60 radiotherapy system. Compared to conventional cardiac imaging at 1.5T and higher, low-field cardiac imaging may have additional benefits including reduced SAR, lower cost, and reduced banding artifacts. In this work, we sought to evaluate the feasibility of a novel bSSFP-EPI technique at 0.35T for cardiac cine imaging. The conventional bSSFP sequence acquires a single echo in each TR. Consequently, the readout duration is approximately one-third of the TR, which is typically 3-4ms, leading to a low acquisition-efficiency2. However, if the bSSFP sequence is modified to acquire multiple echoes from each TR using an echo planar imaging (EPI) strategy, this may increase the acquisition-efficiency2. The major drawback of this approach is increased banding artifacts2 arising from the prolonged TR. However, banding artifacts are reduced at low field strengths, such as 0.35T, and therefore bSSFP-EPI may be feasible at low field strengths to substantially improve the acquisition efficiency without banding artifacts. In this study, we developed a bSSFP-EPI cine sequence and evaluated it on the ViewRay 0.35T MR scanner.Methods
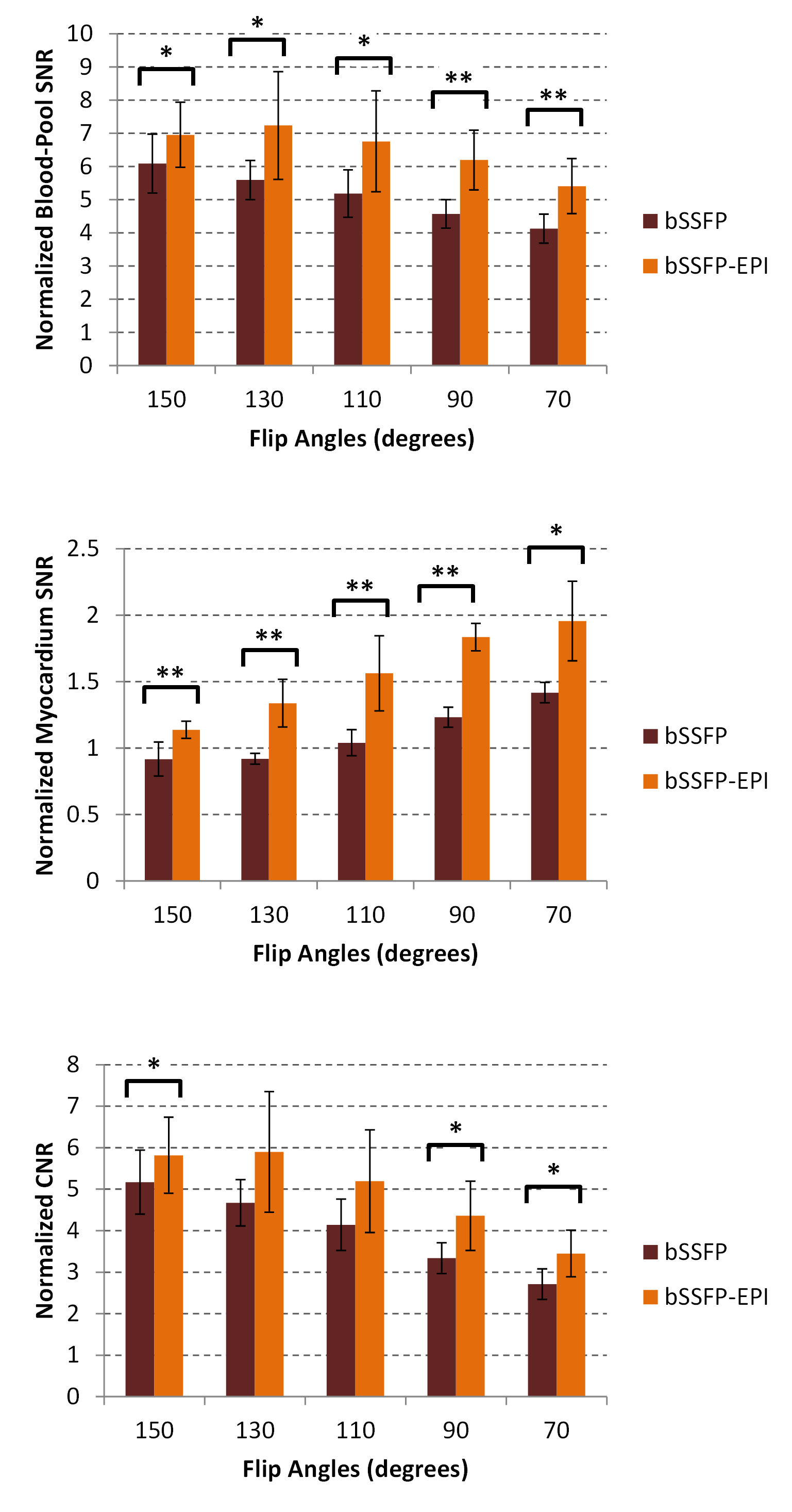
We modified a bSSFP cine sequence to acquire an EPIreadout of 3-7 lines within each TR. The bSSFP-EPI sequence was implemented on the ViewRay 0.35T system and was evaluated in 3 healthy volunteers. Sequence parameters were: TR/TE: 8.1/2.4ms, FOV: 360mm, voxel size: 1.5x1.7x7mm3, readout bandwidth: 772Hz/pixel, flip angles (FA): 70°, 90°, 110°, 130°, 150°. Short axis cine images of the myocardium were acquired. Images were also acquired using a conventional bSSFP cine sequence, with TR/TE: 3.8/1.9 ms (all other parameters were matched). SNR of myocardium and blood pool were calculated from the ratio of the mean tissue intensity to the standard deviation of a background region. Blood-myocardium contrast-to-noise ratio (CNR) was calculated from the difference between the blood-pool SNR and the myocardium SNR. Normalized CNR was calculated by dividing CNR by the square root of acquisition duration. CNR values between bSSFP-EPI and conventional bSSFP images were compared using a paired t-test.Results
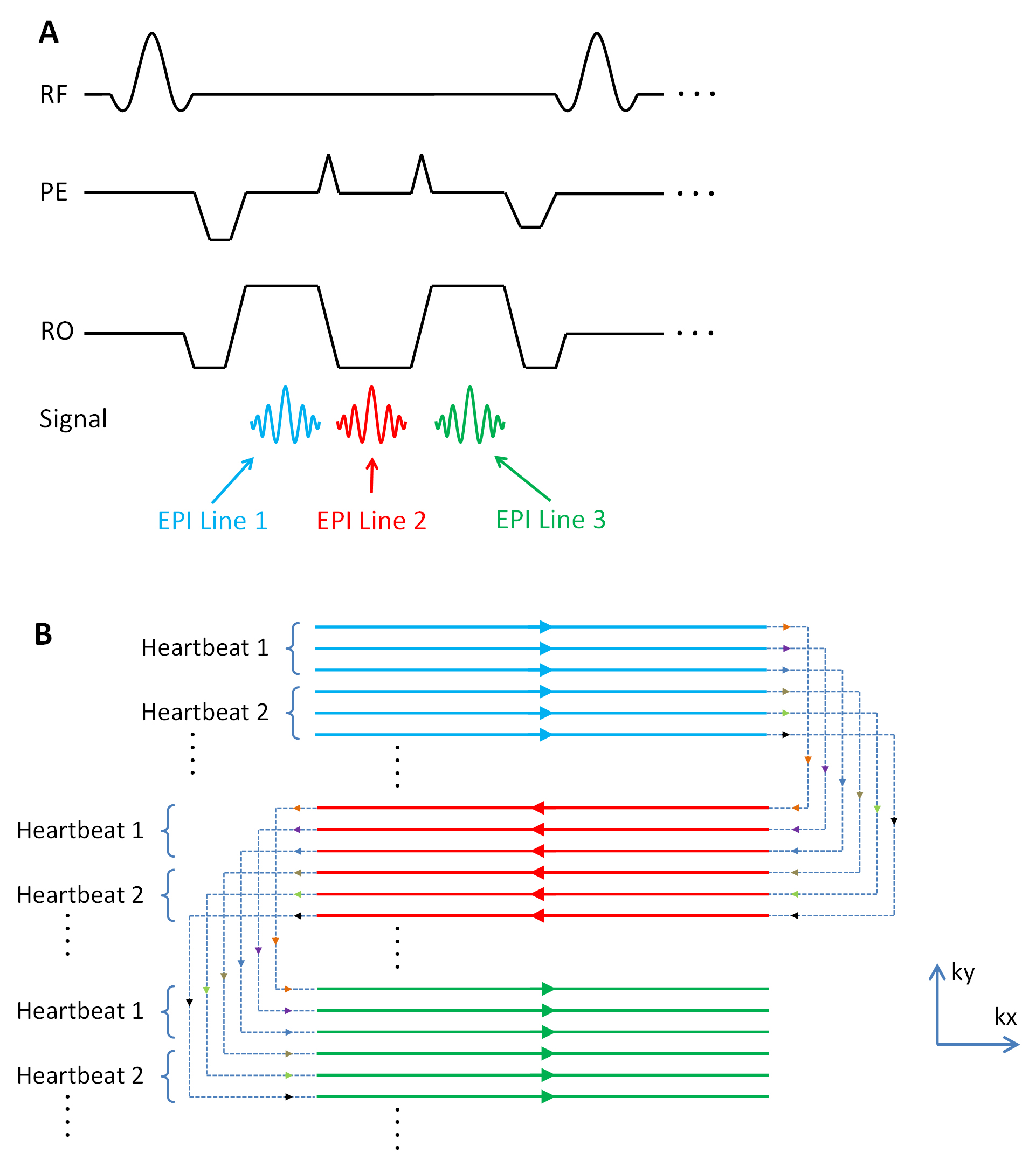
The sequence diagram and readout trajectory for the bSSFP-EPI sequence is shown in Figure 1. The acquisition duration of the bSSFP-EPI cine sequence (3 EPI lines per TR) was 17s (assuming heart rate of 60 beats-per-minute). The corresponding duration for the conventional bSSFP cine sequence was 24s. No parallel imaging was used in any of our imaging acquisition in this study.
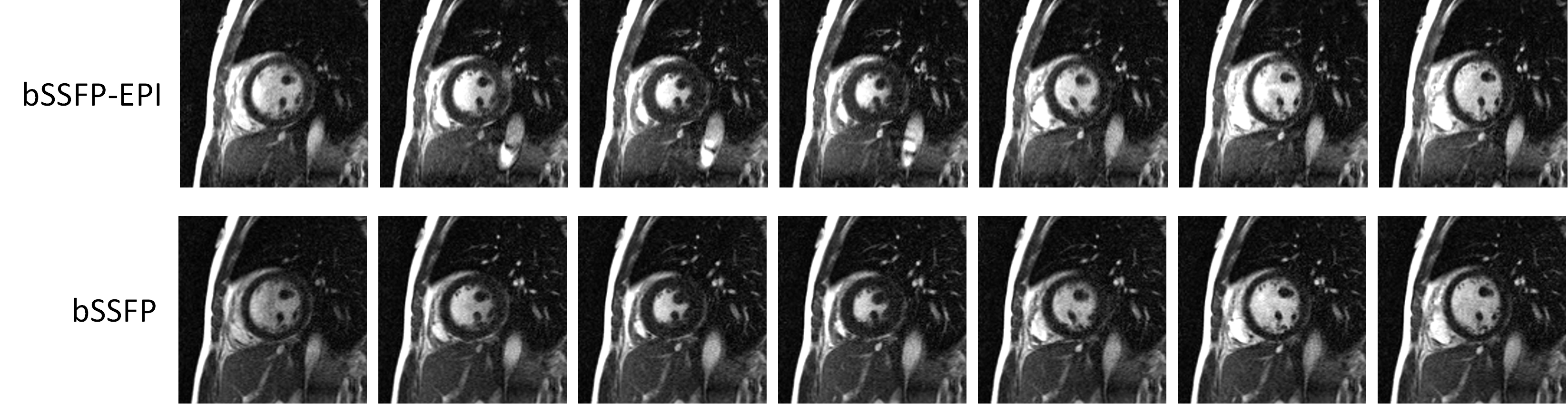
Cine images in a healthy volunteer acquired with bSSFP-EPI cine (3 EPI lines per TR, FA 130°) are shown in Figure 2 top row. Corresponding images acquired with conventional bSSFP cine are shown in Figure 2 bottom row. The bSSFP-EPI provided similar images as conventional bSSFP despite its shorter image acquisition time.
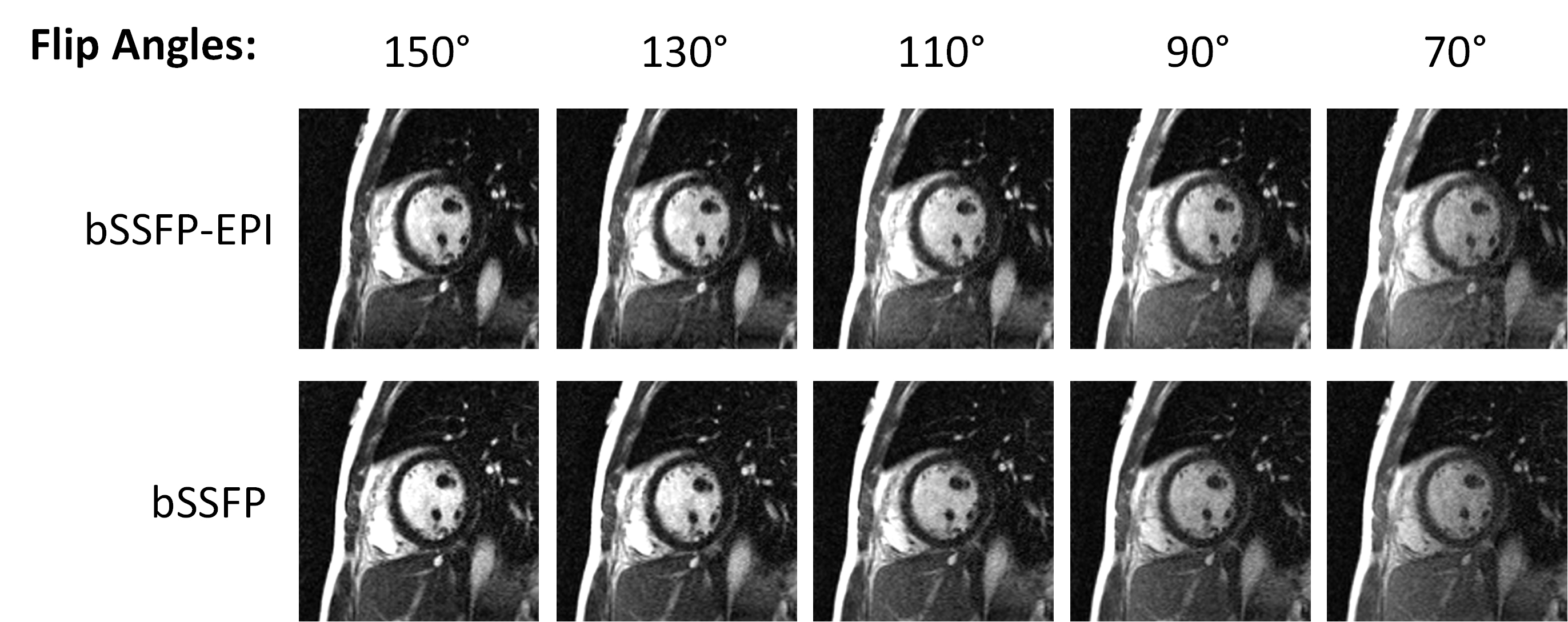
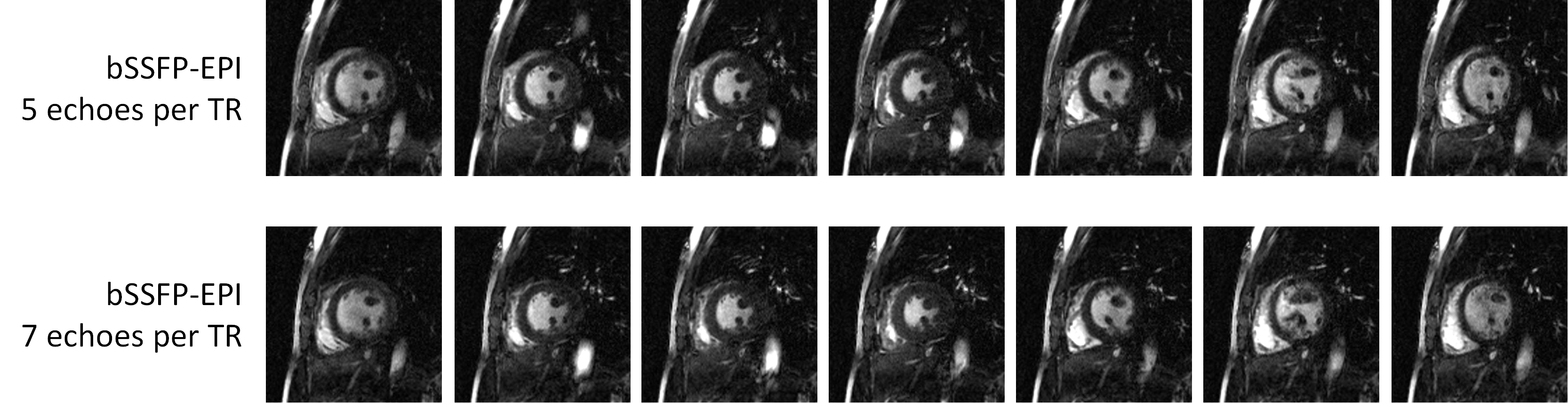
Cine images at multiple flip angles acquired with bSSFP-EPI (3 EPI lines per TR) are shown in Figure 3 top row. Corresponding conventional bSSFP cine images are shown in Figure 3 bottom row. It is apparent that blood-myocardium contrast is higher at larger flip angles. The cine images with up to 150° flip angle was possible due to the dramatically reduced SAR at 0.35T. Cine images acquired with the bSSFP-EPI sequence with 5 and 7 EPI lines per TR are shown in Figure 4. Acquisition duration for both these sequences was 15s.
Normalized blood-pool SNR, myocardium SNR and blood-myocardium CNR values for different FA for bSSFP-EPI (3 EPI lines per TR) and conventional bSSFP images are shown in Figure 5.
Discussion
This study demonstrates the feasibility of a bSSFP-EPI cine sequence on a low-field MRI system. Imaging at a low field such as 0.35T is prone to reduced SNR compared to 1.5T or higher. However, the results show that the myocardium can be clearly delineated, and that the image quality of bSSFP-EPI is similar to that of conventional bSSFP. Our images show in vivo bSSFP-EPI acquisitions with a TR of up to 8.1ms without banding, owing to the lower field strength and improved absolute off-resonance frequencies within the volume of interest. The major advantage of bSSFP-EPI is its reduced acquisition duration, and higher percentage of time per TR used in actual data acquisition, which translated to higher CNR values despite its shorter acquisition time when compared with conventional bSSFP.Conclusion
We have developed a bSSFP-EPI cine sequence and demonstrated its feasibility for diagnostic quality cardiac cine imaging at 0.35T.Acknowledgements
No acknowledgement found.References
1. Finn et al., Cardiac MR imaging: state of the technology, Radiology 241:338 (2006)
2. Herzka et al., Multishot EPI-SSFP in the Heart, MRM 47:655 (2002)
Figures