3275
Feasibility of Cardiac bSSFP Cine MRI at 0.35T: A Comparison with 1.5T1Radiological Sciences, UCLA, Los Angeles, CA, United States, 2Radiological Sciences, University of California, Los Angeles, Los Angeles, CA, United States, 3Radiation Oncology, University of California, Los Angeles, Los Angeles, CA, United States, 4Biomedical Physics Graduate Program, University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
In this study, we demonstrate the feasibility of cardiac cine MRI at 0.35T using bSSFP and compared the results with bSSFP at 1.5T.
Purpose
Although there is presently a strong push for magnetic resonance imaging (MRI) at higher field strengths, clinical cardiac magnetic resonance imaging (MRI) is most frequently carried out at a field strength of 1.5T and less frequently at 3T or higher. While higher field strengths boost the baseline signal-to-noise ratio (SNR), they are often associated with issues such as increased specific absorption rate (SAR), and generally worsening banding artifacts for balanced steady state free precession (bSSFP) sequences. At the other end of the field-strength spectrum, low-field MRI (B0<0.5T) shows promise for diagnostic imaging1,2. Compared to conventional cardiac imaging at 1.5T and higher, low-field cardiac MRI may have additional benefits including reduced SAR, lower cost, reduced banding artifacts and generally shorter tissue T1. Furthermore, due to reduced SAR, low-field MRI may be preferable to higher field strengths for patients with implants and for interventional MR-guided procedures. Our institution recently installed a real-time MRI-guided radiotherapy system (ViewRay Inc., Oakwood Village, OH), which includes a 0.35T superconducting MRI system and a Cobalt-60 radiotherapy system. In this study, we sought to demonstrate the feasibility of cardiac MRI at 0.35T and compare it with cardiac MRI at 1.5T.Methods: Cardiac Cine Imaging
Cardiac cine images were acquired in 6 healthy volunteers at
both 0.35T and 1.5T using a bSSFP cine sequence. Images were acquired for a
range of flip angles (FA) from 50-130°. All parameters were identical at both
field strengths (TR/TE=4/2ms, voxel size 1.25x1.25x7mm3, FOV=320mm,
readout bandwidth 780 Hz/pixel, parallel imaging: GRAPPA). SNR of the
blood-pool and myocardium was calculated from the ratio of the average tissue
signal intensity to the standard deviation of a background region outside the
body. Blood-myocardium contrast-to-noise ratio was calculated from the
blood-pool and myocardium SNR difference. SNR and CNR values at 0.35T were
corrected using the correction factor described below. The k-space data were
all fully sampled and no parallel imaging was used.
Methods: SNR Correction due to RF Coil Difference
Our cardiac MRI was carried out on the ViewRay 0.35T system and on a 1.5T Siemens Avanto system (Siemens Medical Systems, Erlangen, Germany). Because the 0.35T system uses surface receive coils that have been modified to be compatible with the radiotherapy system, we sought to quantify any possible influence on SNR due to coil differences between the 0.35T and 1.5T systems. SNR was measured on both systems in an ACR phantom using a proton-density-weighted FLASH sequence (parameters: TR/TE: 500/3 ms, flip angle (FA): 15°, readout bandwidth: 610 Hz/pixel, voxel size: 1.9x1.9x10mm3) and 30 measurements were acquired. An SNR map was generated by calculating the ratio of the average intensity to the standard deviation over the 30 images on a voxel-by-voxel basis. An average SNR value was then calculated over the entire phantom for each system. If coil performance is identical between the two systems, then SNR ratio of the two systems would be the ratio of the field strengths: 1.5/0.35 = 4.29. However, if the coil performance is not identical, then the SNR values at 0.35T would have to be corrected by a correction factor given by:
Correction factor = (SNR1.5T x 0.35) / (SNR0.35T x 1.5)
Results
The SNR in the ACR phantom was 119.3 at 1.5T and 16.4 at 0.35T, giving a ratio of 7.26 instead of 4.29. Therefore, the SNR values at 0.35T was corrected by a factor of 1.69.
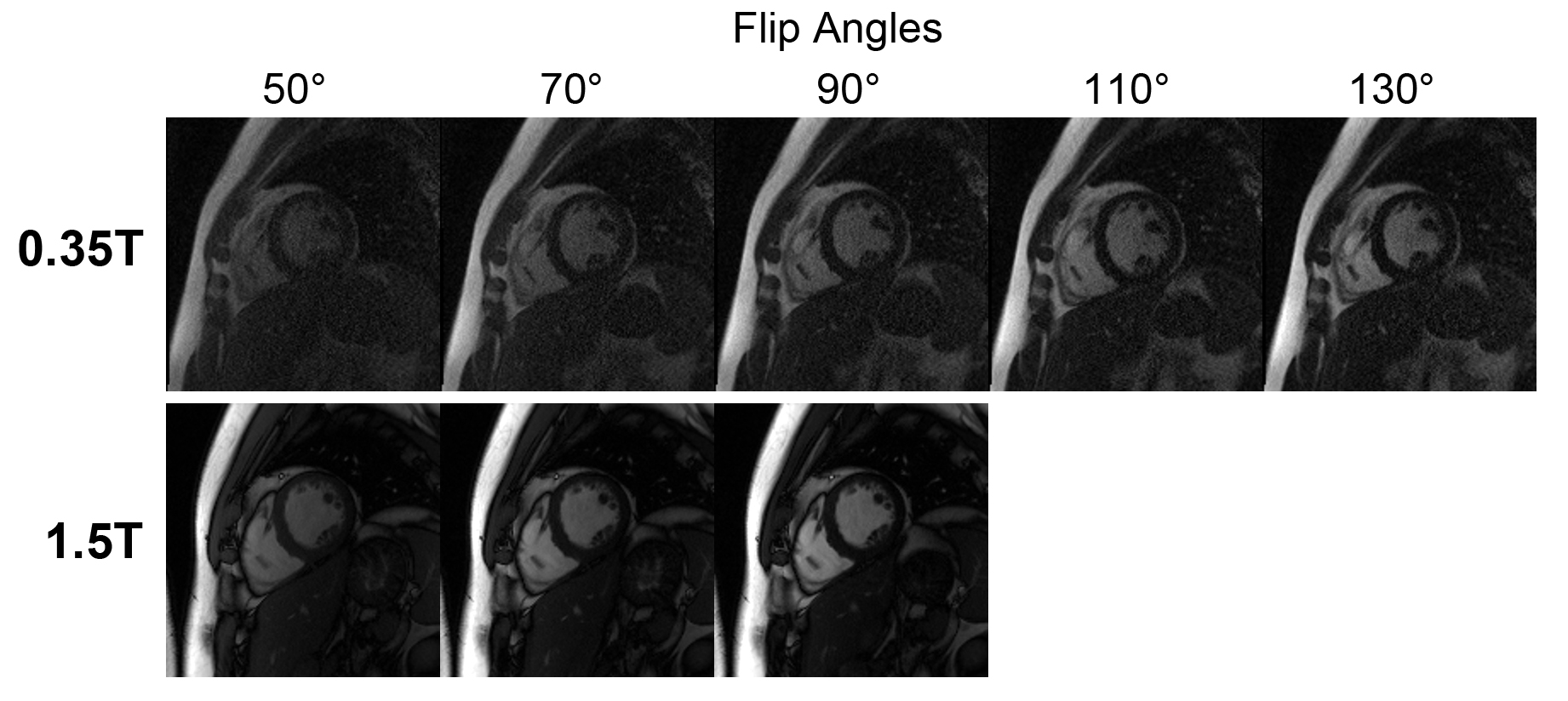
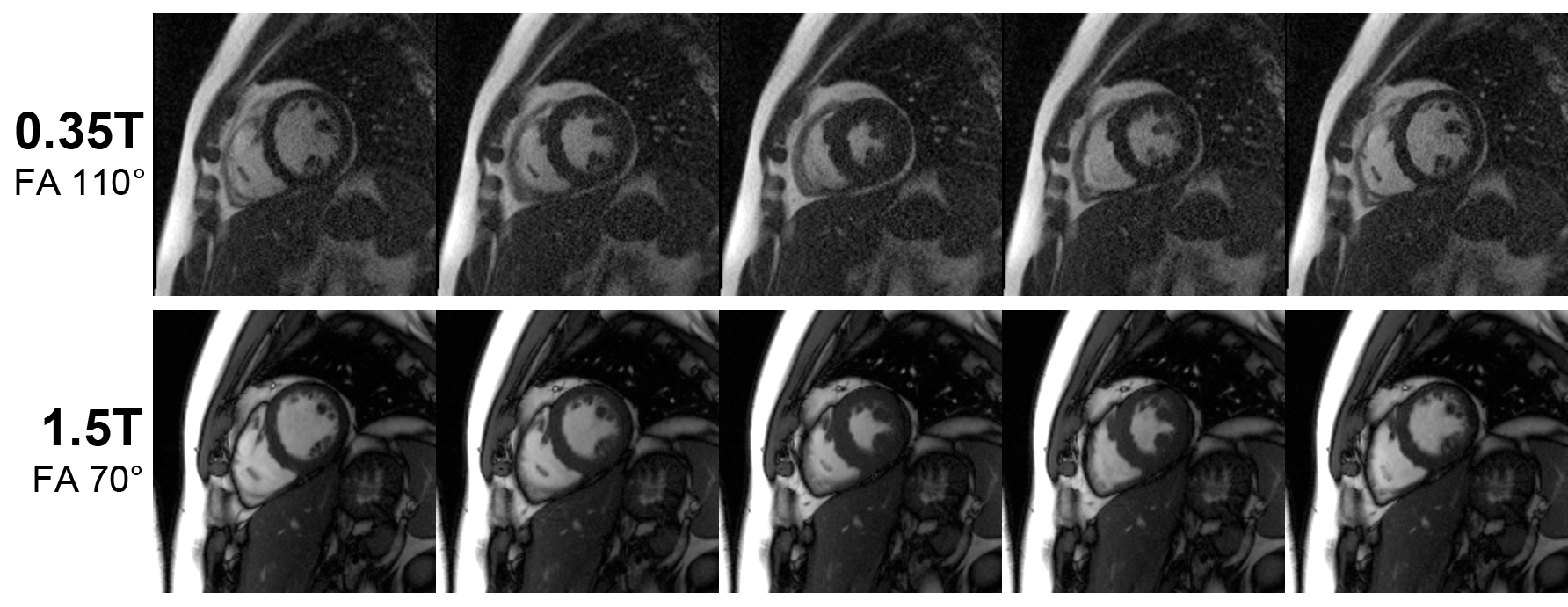
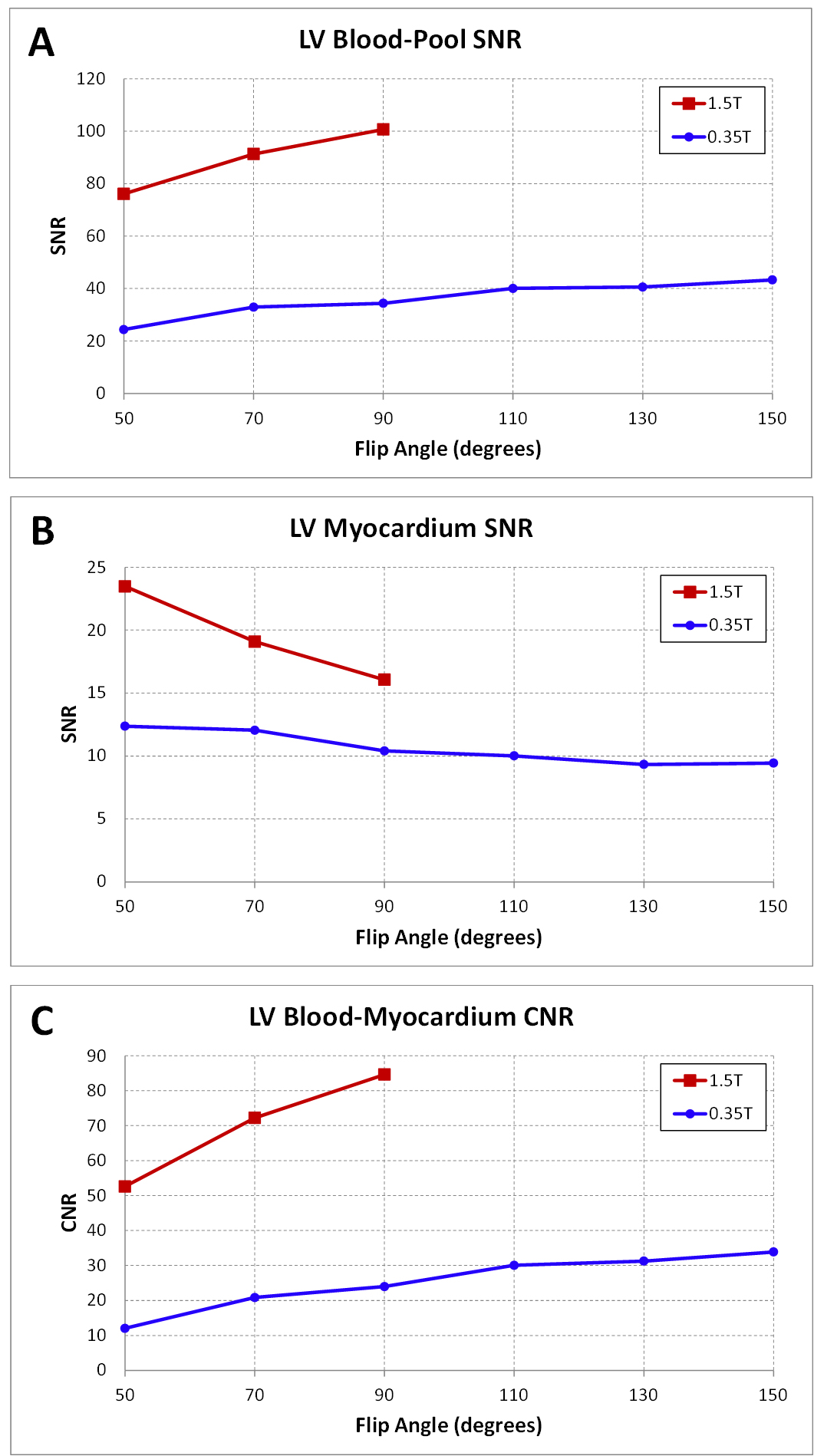
Figure 1 top row shows bSSFP cine images acquired on the 0.35T system for FAs from 50° to 130°. For comparison with cine images at 1.5T, Figure 1 bottom row shows cine images at 1.5T for FAs 50° to 90°. A bSSFP cardiac cine acquisition with FA >90° is generally not possible at 1.5T due to SAR limits. It appears that an FA of about 90° to 110° at 0.35T has improved blood-myocardium contrast and general image quality compared to lower flip angles. Figure 2 shows cine images of multiple cardiac phases at both field strengths. In general, while the 0.35T images appear grainier due to reduced SNR, the left ventricle myocardium walls can be clearly delineated with good contrast. Figure 3 shows the blood-pool SNR, myocardium SNR and blood-myocardium CNR at multiple flip angles in both systems.
Discussion
This study demonstrates that CMR at 0.35T is highly feasible. Due to reduction in SAR, the maximum achievable flip angle for bSSFP cardiac cine imaging is much higher at 0.35T than 1.5T, which allows for improved blood-myocardium contrast. Although the SNR at 0.35T is reduced compared to 1.5T, the quality of the cine images is adequate for diagnostic purposes.Acknowledgements
No acknowledgement found.References
1. Wu et al., PLOS one, May 2016, doi:10.1371/journal.pone.0154711
2. Rutt et al., JMRI, 1996, 1:57-62
Figures