3266
Tomoelastography of the abdominal aorta and inferior vena cava in different hydration states1Charité - Universitätsmedizin Berlin, Berlin, Germany
Synopsis
Tomoelastography was recently introduced for high-resolution stiffness mapping in abdominal organs. The method is based on multifrequency MR elastography and noise-robust reconstruction of shear wave speed maps. This study demonstrates the feasibility of tomoelastography for measurement of the mechanical properties of the abdominal aorta (AA) and inferior vena cava (IVC) in healthy volunteers. AA was measured stiffer than IVC with increasing disparity after drinking one liter of water. Our results demonstrate the sensitivity of MRE-measured effective stiffness values in AA and IVC to physiological alteration of the hydration state and offer a new perspective for MRE of abdominal vessels.
Purpose
Abdominal vessels represent major determining factors for cardiac health. The aortic response to arterial pulse wave pressure influences cardiac afterload while vascular pressure within the abdominal veins such as vena cava influences cardiac preload. So far, vascular pressure cannot directly be measured non-invasively. However, MR elastography (MRE) is capable of measurement of effective vascular stiffness based on fluid motion induced by vibrating vessel walls [1,2]. Since MRE measured effective vascular stiffness is determined by wall stiffness and intra lumen pressure it offers a quantitative imaging marker for the vascular mechanical properties.Methods
We explored the potential of tomoelastography – a recently introduced multifrequency MRE method for high-resolution stiffness mapping in the abdomen [3,4] – to assess the effective stiffness of inferior vena cava (IVC) and abdominal aorta (AA) from 11 shear wave speed maps in a transversal view though the abdomen of 10 healthy volunteers. In a first experiment the volunteers were in a dehydrated state defined by overnight fasting and water abstinence for at least twelve hours. A second experiment was performed 15 min after uptake of 1 liter of water. Multifrequency MRE was performed at 30, 40, 50 and 60 Hz as detailed in [4]. Total measure time was 2 min including four frequencies and full wave field acquisition. Postprocessing was based on tomoelastography, however, with the distinction to [3] of interpolating the spatial resolution of the complex MR images by a factor of 2 to 1.25x1.25 mm² in-plane resolution prior to all further postprocessing steps. Statistical tests were performed using the Wilcoxon's signed rank test and rank sum test for equal medians.Results
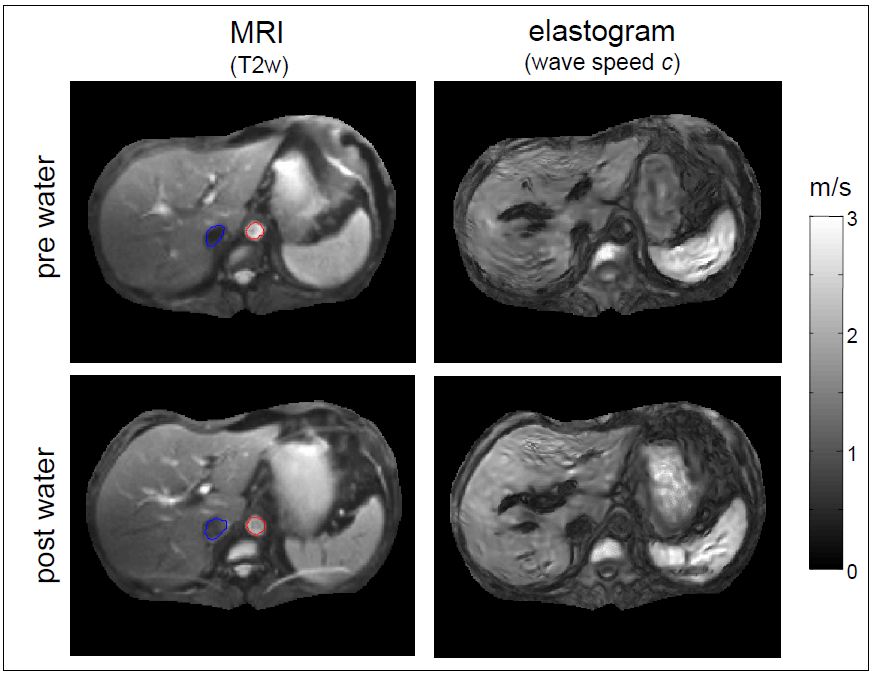
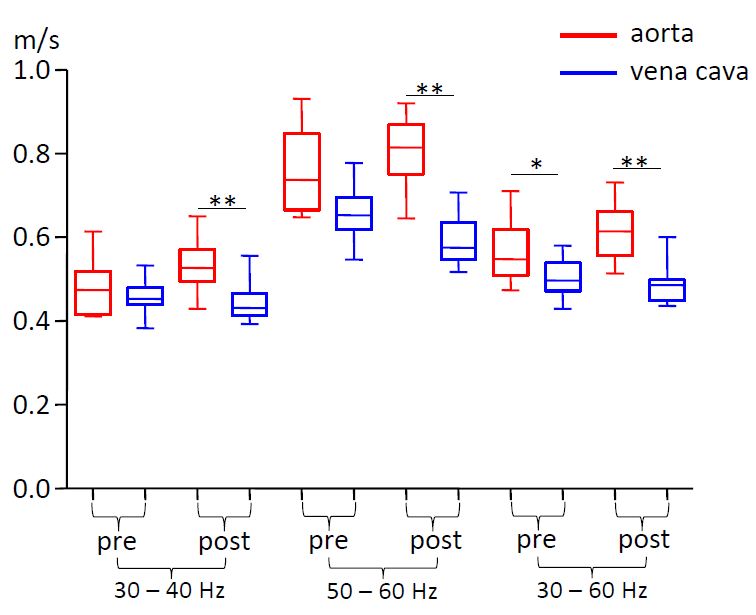
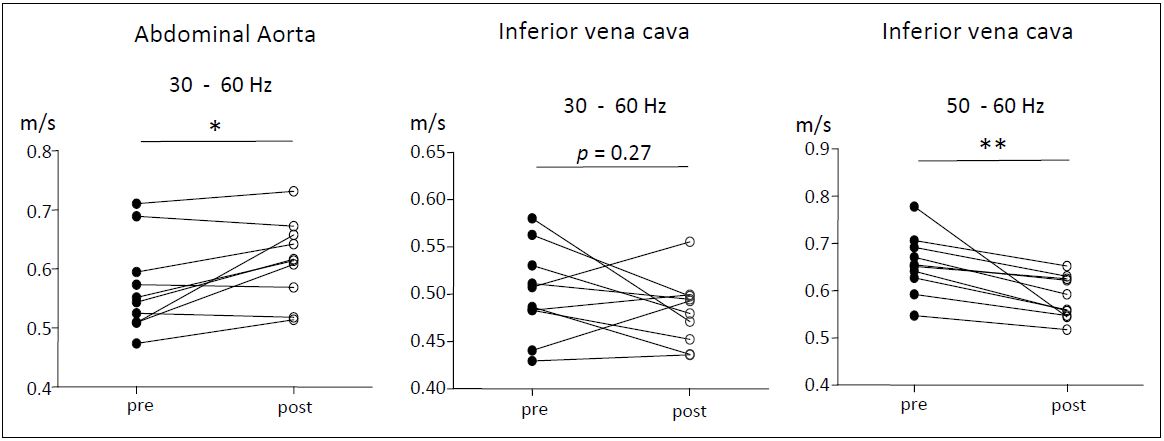
Tomoelastography maps including AA and IVC are shown in figure 1. Organ stiffness in terms of shear wave speed is well visible for the liver, spleen, stomach and intervertebral disk. Regions of AA and IVC are demarcated by blue and red lines, respectively. For further analysis AA- and IVC-stiffness values were averaged within these regions. Figure 2 shows group mean values averaged within the IVC and AA regions pre and post water uptake in different frequency ranges. AA stiffness was higher than IVC stiffness (pre: 568±78 Pa vs. 502±48 Pa, P = 0.019; post: 614±68 Pa vs. 482±36 Pa, P=0.002). Water drinking slightly increased AA stiffness in the full frequency range and reduced CVI stiffness at higher frequencies of 50 and 60 Hz (figure 3). There was only a trend of increase of IVC diameter due to water drinking from 1.6±1.1 to 2.0±1.0 cm² (P=0.06). However, the relative IVC increase was correlated with the relative increase of stiffness (Pearson-r 0.68, P=0.027).Discussion
To our knowledge this is the first MRE study of vascular stiffness of IVC. AA stiffness has been addressed by MRE in multiple studies exploiting a sagittal view through AA at vibration frequency of 60 Hz [1,2]. Our setup covers both AA and IVC, thereby supporting a comparison of both vessels from the same scan. However, due to the transversal image slice orientation our values cannot be compared to the literature. While waveguide effects occur along the main axis of the vessel, an axial view supports measurement of concentrically emanating waves within fluid filled circular cavities such as IVC or AA in a transversal cross section. Irrespective which slice orientation has been chosen, MRE of fluids-filled vessels always deals with both geometry and intrinsic wall properties and measures effective properties rather than intrinsic mechanical constants. Furthermore, our stiffness measurement was not time-resolved across the cardiac cycle. Instead, our study addressed the physiological effect of water uptake on AA and IVC effective stiffness averaged over multiple cardiac cycles. Water drinking was recently reported to influence the stiffness of abdominal organs including the liver, spleen and pancreas [4,5]. There, a higher sensitivity to hydration was observed at higher frequencies than at lower frequencies which is consistent to our findings in IVC but inverse to the observed change in AA. The physiological mechanisms behind the observed disparity of vascular responses to an increased blood volume deserve further investigation.Conclusion
This study demonstrates the feasibility of measuring AA and IVC mechanical properties by tomoelastography showing higher effective stiffness of AA than IVC. The observed stiffness difference increases after water uptake as AA becomes stiffer while IVC becomes softer. The proposed method offers a simple way to assess AA and IVC mechanical properties from conventional abdominal multifrequency MRE scans without additional examinations which potentially increases the clinical value of abdominal MRE.Acknowledgements
No acknowledgement found.References
1. Kenyhercz WE, Raterman B, Illapani VS, Dowell J, Mo X, White RD, Kolipaka A. Quantification of aortic stiffness using magnetic resonance elastography: Measurement reproducibility, pulse wave velocity comparison, changes over cardiac cycle, and relationship with age. Magnetic resonance in medicine 2015.
2. Kolipaka A, Woodrum D, Araoz PA, Ehman RL. MR elastography of the in vivo abdominal aorta: a feasibility study for comparing aortic stiffness between hypertensives and normotensives. J Magn Reson Imaging 2012;35(3):582-586.
3. Tzschatzsch H, Guo J, Dittmann F, Hirsch S, Barnhill E, Johrens K, Braun J, Sack I. Tomoelastography by multifrequency wave number recovery from time-harmonic propagating shear waves. Med Image Anal 2016;30:1-10.
4. Dittmann F, Tzschatzsch H, Hirsch S, Barnhill E, Braun J, Sack I, Guo J. Tomoelastography of the abdomen: Tissue mechanical properties of the liver, spleen, kidney, and pancreas from single MR elastography scans at different hydration states. Magnetic resonance in medicine 2016.
5. Tzschatzsch H, Nguyen Trong M, Scheuermann T, Ipek-Ugay S, Fischer T, Schultz M, Braun J, Sack I. Two-Dimensional Time-Harmonic Elastography of the Human Liver and Spleen. Ultrasound in medicine & biology 2016.
Figures