3263
Fetal cardiac volume reconstruction from motion-corrected multi-slice dynamic MRI1Division of Imaging Sciences and Biomedical Engineering, King's College London, London, United Kingdom, 2Centre for the Developing Brain, King's College London, London, United Kingdom, 3Department of Congenital Heart Disease, King's College LondonEvelina London Children's Hospital, London, United Kingdom
Synopsis
Motion is a significant challenge in fetal cardiac MRI. Multi-slice 2D dynamic MR data was used to reconstruct high-temporal resolution real-time images to be combined in time as 2D cine images and then in space as volumes with full coverage of the heart. Retrospective, image-based post-processing (motion correction, outlier rejection) was used to improve image quality in the presence of intra- and inter-slice motion. Reconstructed multi-slice cine images depict the complex anatomy of the fetal heart across the cardiac cycle and preliminary volume reconstructions allow multiple views to be visualised.
Introduction
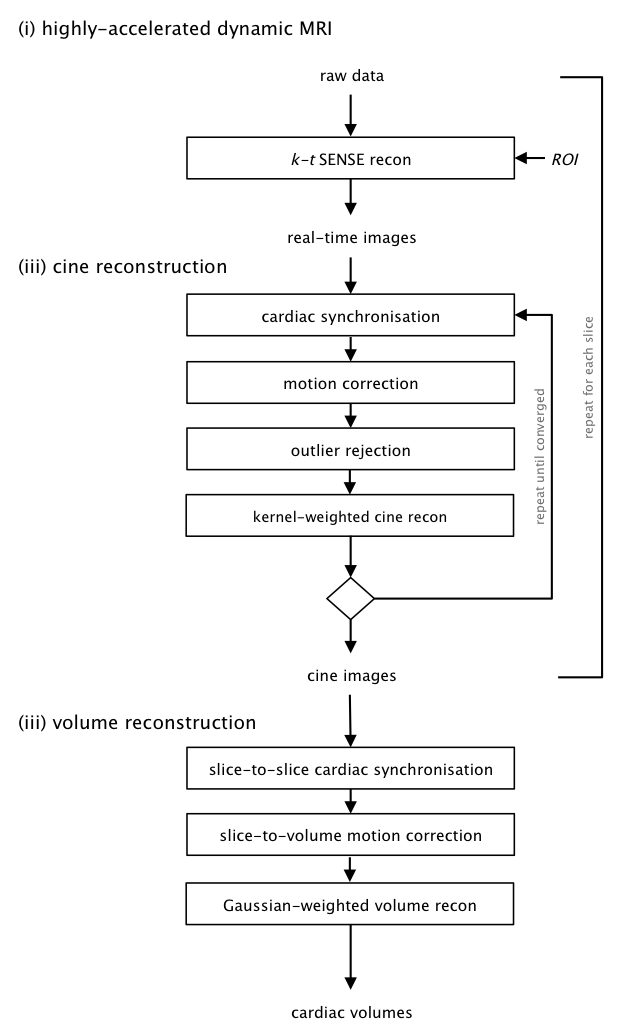
Cardiac MRI is the standard for morphological depiction and functional evaluation of postnatal subjects. However, in utero assessment of the fetal heart and great vessels by MRI is severely limited by motion as the fetal heart has a complex structure, a rapid heart rate, and is a relatively small target for MRI that is displaced by maternal respiration and fetal movements1 . Volumetric MRI of the fetal heart using segmented cine multi-slice short axis acquisition has been achieved2, however, intra- and inter-slice motion remain highly challenging. Two-dimensional cine reconstruction of dynamic MR images, using image-based post-processing for cardiac synchronisation, motion correction and outlier rejection, has shown potential to resolve the beating fetal heart in the presence of motion3. Slice-to-volume reconstruction of 2D snapshot images has proven useful for static volume reconstruction of a variety of fetal organs4,5. In this work, multi-slice 2D dynamic MR data was used to reconstruct high-temporal resolution real-time images to be combined in time as 2D cine images and then in space as volumes with full coverage of the heart (Figure1).Methods
Imaging was performed in four singleton pregnancies (gestational ages 25-30 weeks) on a 1.5 T Philips Ingenia without maternal breath-hold using an anterior torso coil array in combination with a posterior spine coil array. Multi-slice dynamic data was acquired in short and long axis orientations using a 2D bSSFP sequence with regular Cartesian k-t undersampling (TR/TE 4.4/2.2 ms, flip angle 60°, field of view 400 × 304 mm, voxel size 2.0 × 2.0 x 6.0 mm, slice overlap 3 mm, 8 s per slice). A low spatial resolution SSFP localiser was used for scan planning. Operation was constrained to less than 2 W/kg whole body SAR, and low PNS and gradient-induced acoustic noise settings were used, necessarily limiting scanner performance. A user-specified fetal heart region-of-interest (ROI) was the only manual preparation required for reconstruction.
The fetal heart in utero is surrounded by the fetal body, uterus, and maternal torso. This discrepancy in size and temporal dynamics of the fetal heart and surrounding anatomy leads to highly complementary signal properties in space and time, with the fetal heart occupying only a small fraction of the spatial field of view, but exhibiting a large range of temporal frequencies.Dynamic imaging with 2D k-t under-sampling was used and, taking advantage of this spatiotemporal sparsity, real-time images were reconstructed using k-t SENSE6 with spatially-varying regularisation to preferentially capture the higher temporal content in the fetal heart ROI, at the cost of increased noise.
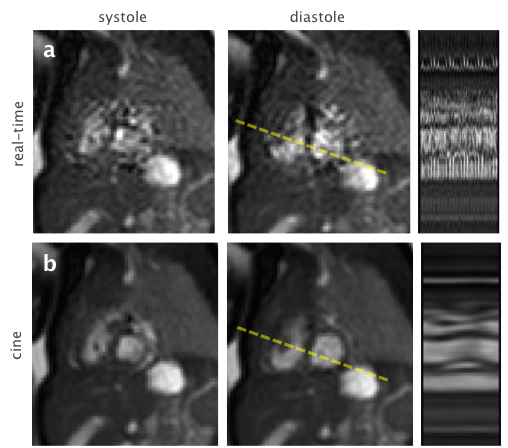
Temporal kernel-weighted interpolation was used to combine the 2D real-time images into a set of cine images with improved SNR (Figure2). A sinc kernel with periodicity corresponding to the frequency truncation of the k-t SENSE reconstruction was used, with Tukey windowing for continuity in cyclic cardiac time. Image-based self-gating and registration was used to align the spatial location and cardiac phase of the fetal heart between images prior to interpolation2, and outlier rejection was included as a robust statistic in the kernel-weighting function to down-weight both voxels corrupted by motion artefact and real-time images containing inconsistent anatomical views.
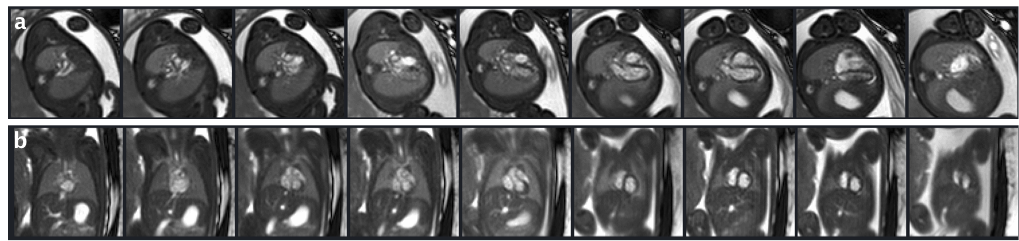
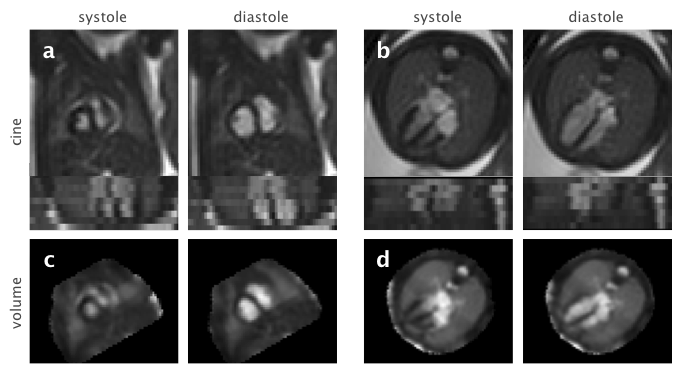
For volume reconstruction, the cardiac cycle was synchronised between pairs of adjacent slices using cross-correlation of the image intensities in the ROI (Figure3). Cine images were combined using a slice-to-volume approach to correct inter-slice movement7. The localiser scan was used as a target for image registration and cines were initially registered as stacks and then as individual slices. Volume reconstruction was performed using a Gaussian point-spread-function in the through-slice direction (Figure4).
Results & Discussion
Highly-accelerated real-time imaging was able to capture the motion of the fetal heart as well as the surrounding anatomy, allowing for direct estimation of and correction for cardiac pulsation and motion. Cine reconstruction effectively combined the data as a single cardiac cycle, increasing the visibility of dynamic anatomical features. The use of robust statistics enabled the reconstruction to effectively deal with inconsistencies in the data, such as maternal respiration, motion artefact, and short episodes of fetal movement. Multi-slice cine images depict the complex anatomy of the fetal heart across the cardiac cycle and preliminary volume reconstructions allow multiple views to be visualised (e.g. the short and long axis planes shown in Figure 4). The proposed method shows promise as a framework for comprehensive fetal cardiac MRI. Future work will aim to extend to a full volumetric reconstruction capable of accommodating a much wider range of fetal motion than the current hybrid approach. Overcoming the key challenge of motion will enable further detail in studies of the fetal heart.Acknowledgements
This research was supported by the EPSRC Programme, the MRC Strategic Fund, the Wellcome Trust iFIND project, and by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy's and St Thomas' NHS Foundation Trust and King's College London. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.References
1. Votino C, Jani J, Damry N, Dessy H, Kang X, Cos T, Divano L, Foulon W, De Mey J, Cannie M. Magnetic resonance imaging in the normal fetal heart and in congenital heart disease. Ultrasound in Obstetrics & Gynecology 2012;39:322–9. doi: 10.1002/uog.10061.
2. Roy C, Seed M, Macgowan C, Roy C, Feng L. High resolution multislice imaging of the fetal heart using iGRASP and MOG. JCMR. 2016;18:P44. doi: 10.1186/1532-429X-18-S1-P44.
3. van Amerom JFP, Kuklisova Murgasova M, Price AN, et al. Fetal cardiac cine imaging from super-resolution reconstruction of highly-accelerated real-time MRI. ISMRM. 2016;458.
4. Kuklisova-Murgasova M, Quaghebeur G, Rutherford MA, Hajnal JV, Schnabel JA. Reconstruction of fetal brain MRI with intensity matching and complete outlier removal. Medical image analysis 2012;16:1550–64. doi: 10.1016/j.media.2012.07.004.
5. Lloyd DFA, Kainz B, van Amerom JFP, Pushparajah K, John M. Three-Dimensional Modelling of the Fetal Vasculature from Prenatal MRI using Motion-Corrected Slice-to-Volume Registration. ISMRM 2016:1677.
6. Tsao J, Boesiger P, Pruessmann KP. k-t BLAST and k-t SENSE: dynamic MRI with high frame rate exploiting spatiotemporal correlations. Magnetic Resonance in Medicine 2003;50:1031–42. doi: 10.1002/mrm.10611.
7. Jiang S, Member S, Xue H, Glover A, Rutherford M, Rueckert D, Hajnal J V. MRI of moving subjects using multislice Snapshot images with Volume Reconstruction (SVR): Application to fetal, neonatal, and adult brain studies. IEEE Trans. Med. Imaging 2007;26:967–980.
Figures