3255
High Resolution, Single-shot LGE MRI with Compressed Sensing and Radial k-space Sampling1Biomedical Engineering, Northwestern University, Chicago, IL, United States, 2Radiology, Northwestern university, Chicago, IL, United States, 3Division of Cardiology, Internal Medicine, Northwestern University, Chicago, IL, United States
Synopsis
We sought to develop a high resolution single-shot LGE pulse sequence using Radial Compressed Sensing. We then evaluated in patients the performance of our acquisition scheme with respect to segmented clinical LGE.
Introduction
Late gadolinium enhanced (LGE)1-3 is considered the gold standard test for assessment of myocardial viability. LGE MRI is typically administered in two different ways: (i) segmented, breath-held (BH) acquisition with gradient echo readout and (ii) single-shot, free-breathing acquisition with balanced steady-state free precession (b-SSFP) readout. While a breath-hold LGE acquisition provides higher spatial resolution than a single-shot LGE acquisition, it requires longer scan time and is sensitive to arrhythmia and breathing motion. While a single-shot LGE acquisition can be conducted during free-breathing and is insensitive to arrhythmia, it provides lower spatial resolution than a segmented, breath-hold LGE acquisition. Compressed sensing (CS)4 is revolutionizing cardiovascular MRI with unprecedented imaging speed. A previous study using 3D LGE with CS5 showed that high spatial resolution improves scar quantification and identification of grey zones. We sought to develop and evaluate a single-shot LGE pulse sequence with spatial high resolution using CS and radial k-space sampling.Method
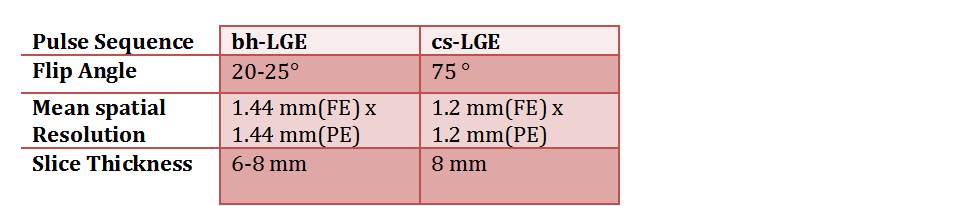
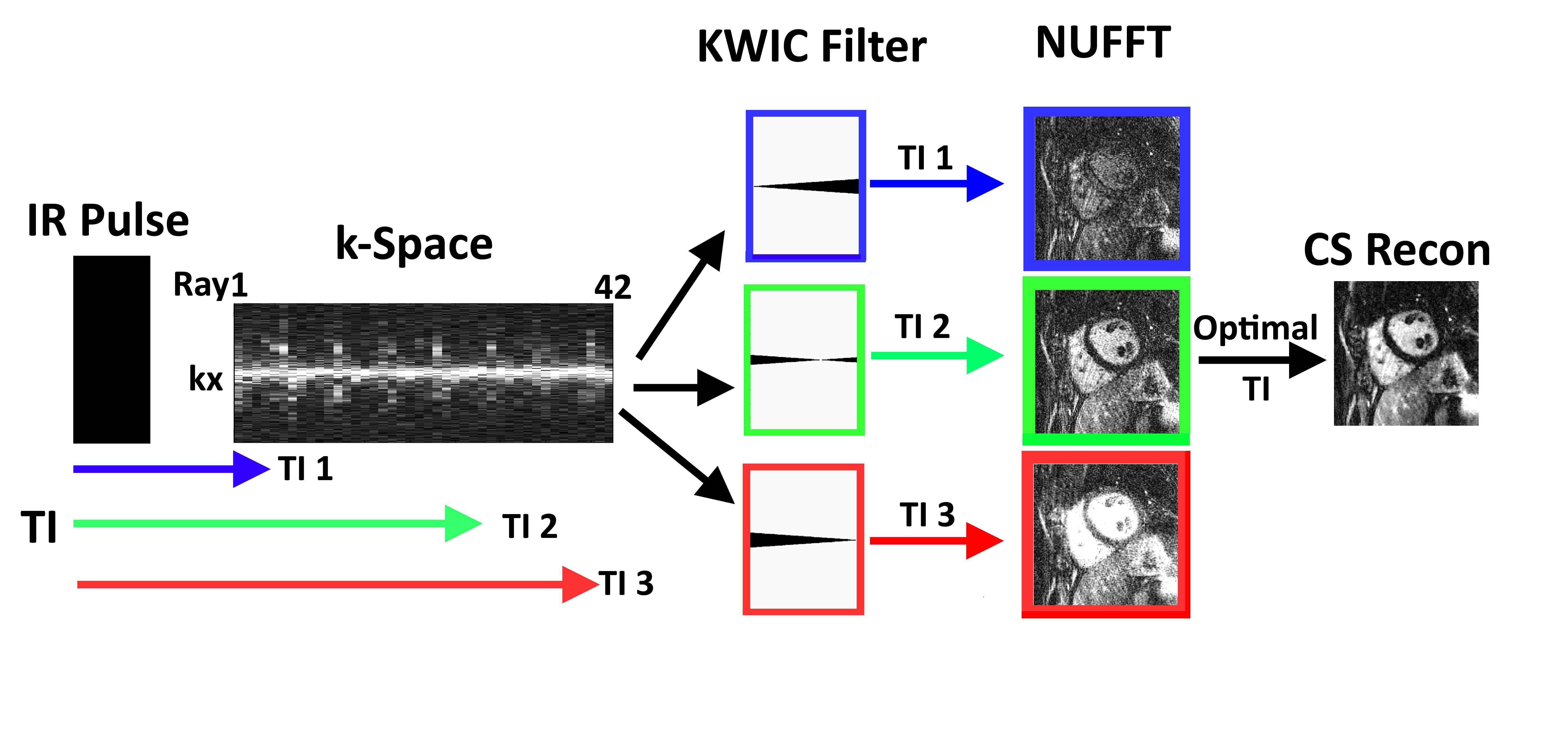
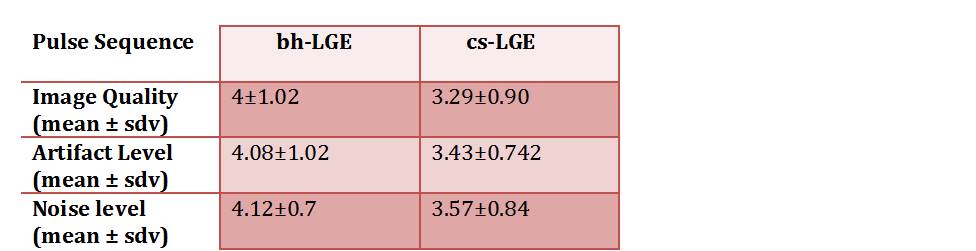
(Patient) We enrolled 14 patients (mean age = 57.14 ± 15.7 years; 5 males; 9 females) who were scheduled to undergo clinical cardiovascular MRI, which included clinical BH LGE as reference. (Image Acquisition) Single-shot LGE pulse sequence with CS and radial k-space sampling was implemented on 1.5T (Avanto, Aera, Siemens) and 3T (Skyra, Siemens) scanners. Relevant image parameters are summarized in Table 1. Note that radial scans acquired 42 radial rays with the 5th Golden angle sequence6. To suppress streak artifacts arising from k-space undersampling, particularly in outer volume regions, we used a wideband inversion pulse7. Single-shot LGE with CS was conducted immediately after clinical LGE to sample a stack of short-axis planes. (Image reconstruction) We used the k-space weighted image contrast (KWIC) filter8, 9 to choose a unique inversion time (TI) for LGE reconstruction. As shown in Fig. 1, this scheme enabled us to identify an optimal TI retrospectively and eliminate a need to perform PSIR reconstruction10. After identifying an optimal TI, we removed aliasing artifact using CS with spatial total variation (TV)4 with 100 iterations and normalized regularization weight of 0.000025. (Data Analysis) With clinical segmented, BH LGE as reference, we compared the image quality of single-shot LGE with CS (spatial TV and TGV). 26 short-axis stacks (12 clinical LGE, 14 CS LGE) were randomized and evaluated by 2 readers in a blinded, independent fashion for the following three categories using a 5-point Likert scale: image quality, artifact level, and noise level. Note that an entire short-axis stack received one score. An average score of ≥ 3.0 was considered to be diagnostically acceptable. Qualitative scores were compared using Wilcoxon signed rank test.Results
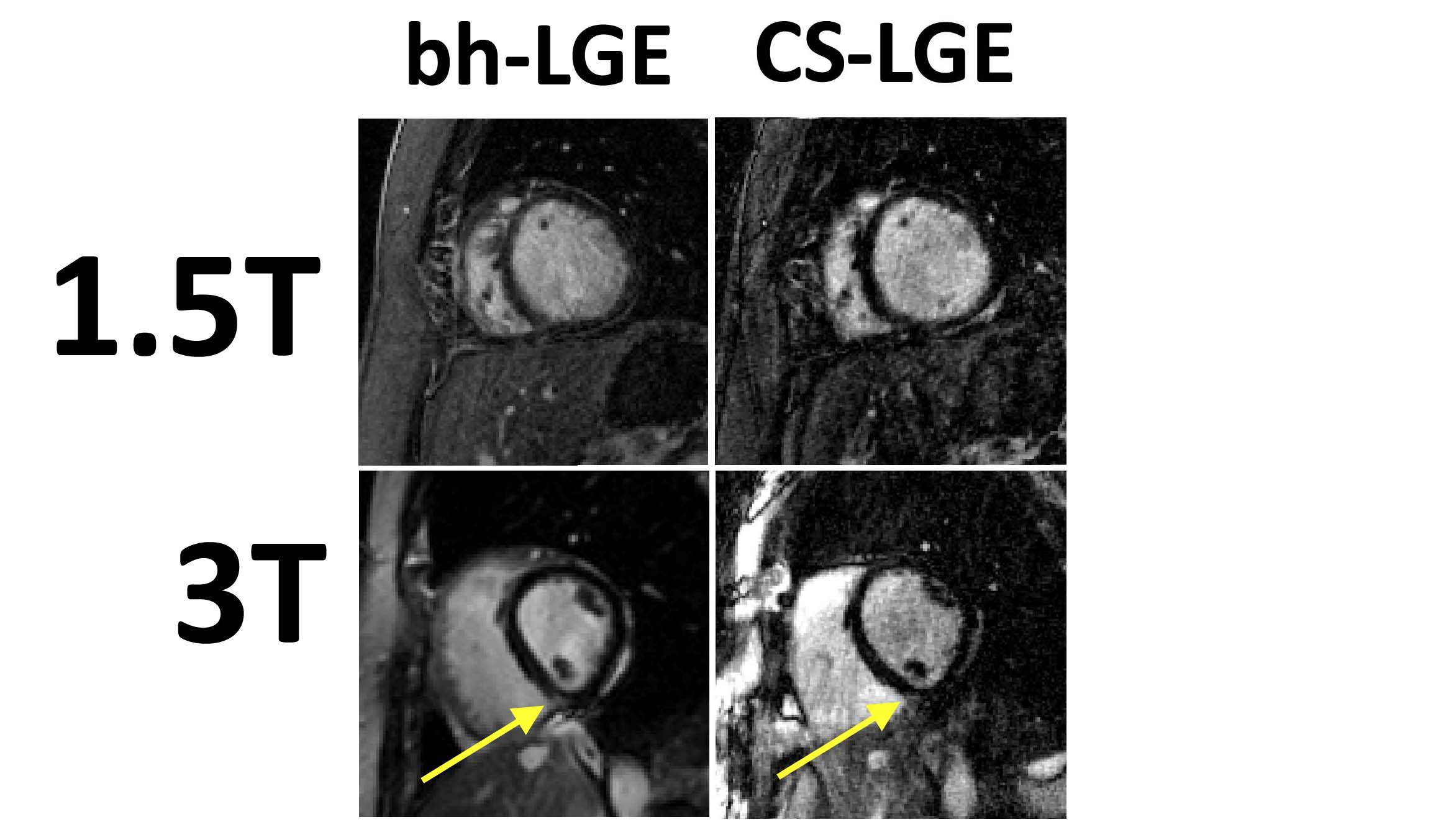
Figure 2 shows representative quality produced by clinical segmented, breath-hold LGE and single-shot LGE with CS scans at 1.5T and 3T. Table 2 summarizes the image quality scores. Averaging the results over 14 patients, the readers’ scores were not significantly different for all categories.Discussion
This
study demonstrates that a combination of CS and radial k-space sampling
produces single-shot LGE images with high spatial resolution and image quality.
A future study is warranted to rigorously evaluate the diagnostic performance of
single-shot LGE with CS in patients with myocardial scars. Acknowledgements
This work was supported by NIH Grant 1R01HL116895-01A1.
References
1. Kim RJ, Fieno DS, Parrish TB, Harris K, Chen EL, Simonetti O, Bundy J, Finn JP, Klocke FJ, Judd RM. Relationship of mri delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation. 1999;100:1992-2002
2. Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, Klocke FJ, Bonow RO, Judd RM. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000;343:1445-1453
3. Simonetti OP, Kim RJ, Fieno DS, Hillenbrand HB, Wu E, Bundy JM, Finn JP, Judd RM. An improved mr imaging technique for the visualization of myocardial infarction. Radiology. 2001;218:215-223
4. Lustig M, Donoho D, Pauly JM. Sparse mri: The application of compressed sensing for rapid mr imaging. Magnetic Resonance in Medicine. 2007;58:1182-1195
5. Akcakaya M, Rayatzadeh H, Basha TA, Hong SN, Chan RH, Kissinger KV, Hauser TH, Josephson ME, Manning WJ, Nezafat R. Accelerated late gadolinium enhancement cardiac mr imaging with isotropic spatial resolution using compressed sensing: Initial experience. Radiology. 2012;264:691-699
6. Wundrak S, Paul J, Ulrici J, Hell E, Rasche V. A small surrogate for the golden angle in time-resolved radial mri based on generalized fibonacci sequences. IEEE transactions on medical imaging. 2015;34:1262-1269
7. Ranjan R, McGann CJ, Jeong EK, Hong K, Kholmovski EG, Blauer J, Wilson BD, Marrouche NF, Kim D. Wideband late gadolinium enhanced magnetic resonance imaging for imaging myocardial scar without image artefacts induced by implantable cardioverter-defibrillator: A feasibility study at 3 t. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2015;17:483-488
8. Song HK, Dougherty L. K-space weighted image contrast (kwic) for contrast manipulation in projection reconstruction mri. Magn Reson Med. 2000;44:825-832
9. Winkelmann S, Schaeffter T, Koehler T, Eggers H, Doessel O. An optimal radial profile order based on the golden ratio for time-resolved mri. IEEE transactions on medical imaging. 2007;26:68-76
10. Kellman P, Arai AE, McVeigh ER, Aletras AH. Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magn Reson Med. 2002;47:372-383
Figures