3254
Ungated free-breathing late gadolinium enhancement imaging with a radial simultaneous multi-slice acquisition1Radiology and Imaging Sciences, University of Utah, Salt lake city, UT, United States, 2Cardiology, University of Utah, Salt Lake City, UT, United States
Synopsis
Late Gadolinium Enhancement imaging is the gold standard for identifying infarcted myocardium. Existing data acquisition methods rely on good ECG-gating signal and breathholding to acquire images in quiescent diastolic cardiac phase. However, in patients with arrhythmias and when imaging at higher field strengths, R-R interval is inconsistent and a good ECG signal can be challenging. This can lead to increased acquisition time and inconsistent recovery of longitudinal magnetization affecting signal-to-noise ratio and optimal myocardial nulling. Here we propose an ungated free-breathing scheme that acquires multiple slices at the same time with consistent nulling of healthy myocardium at systole and diastole.
Purpose
To develop an ungated free-breathing Late Gadolinium Enhancement(LGE) imaging framework with accelerated slice coverage using a simultaneous multi-slice acquisition. LGE imaging is the gold standard for identifying infarcted myocardium [1, 2]. Conventional LGE imaging involves acquiring data in a segmented fashion over several breathholds and can take 10-15 seconds per slice [3]. Single shot methods that acquire an entire image with in one heart beat have also been proposed [4, 5]. However conventional and single shot methods can suffer when the ECG gating is poor or in the case of arrhythmias. The acquisition time can be increased with the conventional acquisitions potentially causing ghosting artifacts[6]. Changing R-R intervals can cause inconsistent recovery of the longitudinal magnetization and can affect image quality in terms of signal to noise ratio and sub-optimal nulling of the normal myocardium. Ungated LGE imaging offers a simplified acquisition scheme and can overcome these issues. Ungated imaging was originally proposed in[7] where an inversion pulse was intermittently applied and images were acquired continuously after an inversion recovery time. The ungated approach was also extended to black blood LGE imaging[6]. However, these methods[6,7] acquire one slice at a time and lead to varying contrasts between normal and infarcted myocardium across cardiac phases. Here we propose an ungated LGE scheme with slice acceleration using a radial simultaneous multi-slice (SMS) technique. SMS imaging excites and acquires multiple slices at the same time and promising results have been shown in cardiac cine and perfusion imaging[8-10]. The proposed LGE method with SMS leads to consistent image contrast between normal and infarcted myocardium for all cardiac phases.Methods
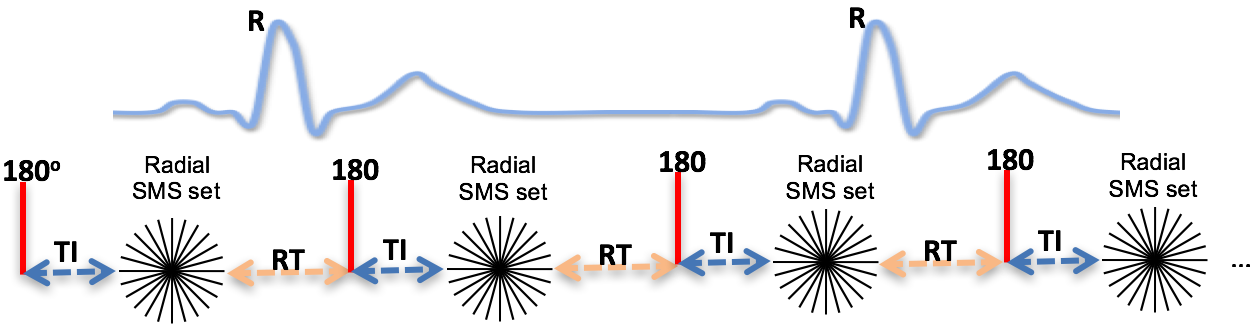
The ungated LGE acquisition scheme is shown in Figure 1. After an inversion pulse and an inversion recovery time, TI, to null the healthy myocardium, radial SMS data were acquired. Three short-axis slices were acquired simultaneously. The process was repeated after a longitudinal magnetization recovery time (RT). Undersampled radial SMS data was acquired on a Siemens 3T Prisma scanner using a 32 channel torso coil. The scan parameters were TR=2.3 msec, TE=1.3 msec, slice thickness=8mm, flip angle=20°, FOV=260 mm2. Matrix size=176 x 36 (readout x number of rays), RT=800 msec. TI was determined using a TI-scout sequence. A total Gadolinium dose of 0.15 mmol/kg (Prohance) was given 10 minutes before the start of LGE imaging. The ungated LGE sequence was run continuously for a minute in a normal subject and in a subject with a known infarct.
Reconstruction of the radial SMS data was performed using a joint multi-slice spatio-temporal total variation constrained reconstruction (STCR)[9] by minimizing C in equation(1).
$$C(I)={\sum^{nc}_{i=1}{\left\|\left(\sum^{nsl}_{j=1}{{\phi }_j}\left(GS_{ij}I_j\right)\right)-d_i\right\|}}^2_2+\:{\alpha }_t\sum^{nsl}_{j=1}{{TV}_t}\left(I_j\right)+\:{\alpha }_s\sum^{nsl}_{j=1}{{TV}_s}\left(I_j\right)\:\:\:\:\:(1)$$
In equation(1),$$$d_i$$$ is the acquired data for coil $$$i$$$, $$$nc$$$ is the number of coils, $$$I_j$$$ is the image estimate for slice $$$j$$$, $$$nsl$$$ is the number of simultaneously excited slices, $$$S_{ij}$$$ is the coil-sensitivity for coil $$$i$$$ and slice $$$j$$$, $$$\phi_j$$$ phase modulates k-space data for slice $$$j$$$ (for a slice acceleration factor of three this corresponds to alternating phase modulation with phases $$$0$$$,$$$2pi/3$$$,$$$4pi/3$$$), and $$$G$$$ is the gridding operator to convert image data to radial k-space data. $$$TV_t$$$ and $$$TV_s$$$ are the temporal and spatial total variation constraints [11].
A preliminary STCR reconstruction with 25 iterations was first performed in order to retrospectively bin the data into near systolic and near diastolic cardiac phases. A region of interest encompassing the heart was drawn and the summed signal in the region was used for self-gating the data[12, 13]. Local peaks in the self-gating signal were identified as near diastole and local minima as near systole. Final STCR reconstruction for each cardiac phase was done separately in order to reduce the effect of cardiac motion.
Results
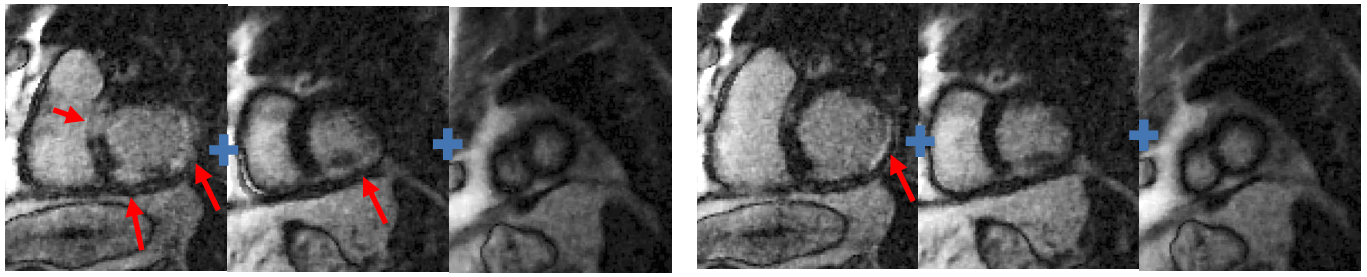
Figure 2 shows the results for one radial SMS set at near systole and at near diastole in a normal subject. The plus signs between the images indicate that the slices are simultaneously acquired. Figure 3 shows the results in a subject with known infarct. Regions with myocardial infarction are pointed by arrows.Discussion and Conclusion
Ungated free-breathing LGE imaging with radial SMS is a simpler and promising alternative to conventional acquisitions that rely on good ECG signal and breathholding. Since 36 rays are acquired in ~83 msec, proposed method potentially minimizes intra-frame blurring/ghosting due to cardiac motion as compared to single shot schemes[4]. While one SMS set is acquired here, complete LV coverage can be obtained by interleaving multiple SMS sets. The radial acquisition scheme is robust to intra and inter-time frame motion and can lead to improved visualization and quantification of scar volume at systole and diastole.Acknowledgements
No acknowledgement found.References
[1] R.J. Kim, D.S. Fieno, T.B. Parrish, K. Harris, E.L. Chen, O. Simonetti, J. Bundy, J.P. Finn, F.J. Klocke, R.M. Judd, Relationship of MRI delayed contrast enhancement to irreversible injury, infarct age, and contractile function, Circulation, 100 (1999) 1992-2002.
[2] O.P. Simonetti, R.J. Kim, D.S. Fieno, H.B. Hillenbrand, E. Wu, J.M. Bundy, J.P. Finn, R.M. Judd, An Improved MR Imaging Technique for the Visualization of Myocardial Infarction, Radiology, 218 (2001) 215-223.
[3] R.J. Kim, E. Wu, A. Rafael, E.L. Chen, M.A. Parker, O. Simonetti, F.J. Klocke, R.O. Bonow, R.M. Judd, The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction, The New England journal of medicine, 343 (2000) 1445-1453.
[4] W. Li, B.S.Y. Li, J.A. Polzin, V.M. Mai, P.V. Prasad, R.R. Edelman, Myocardial delayed enhancement imaging using inversion recovery single-shot steady-state free precession: Initial experience, Journal of Magnetic Resonance Imaging, 20 (2004) 327-330.
[5] A. Huber, S.O. Schoenberg, B. Spannagl, J. Rieber, I. Erhard, V. Klauss, M.F. Reiser, Single-Shot Inversion Recovery TrueFISP for Assessment of Myocardial Infarction, American Journal of Roentgenology, 186 (2006) 627-633.
[6] J.S. Detsky, J.J. Graham, R. Vijayaraghavan, L. Biswas, J.A. Stainsby, M.A. Guttman, G.A. Wright, A.J. Dick, Free-breathing, nongated real-time delayed enhancement MRI of myocardial infarcts: A comparison with conventional delayed enhancement, Journal of Magnetic Resonance Imaging, 28 (2008) 621-625.
[7] M.A. Guttman, A.J. Dick, V.K. Raman, A.E. Arai, R.J. Lederman, E.R. McVeigh, Imaging of myocardial infarction for diagnosis and intervention using real-time interactive MRI without ECG-gating or breath-holding, Magnetic Resonance in Medicine, 52 (2004) 354-361.
[8] D. Stäb, T. Wech, F.A. Breuer, A.M. Weng, C.O. Ritter, D. Hahn, H. Köstler, High resolution myocardial first-pass perfusion imaging with extended anatomic coverage, Journal of Magnetic Resonance Imaging, 39 (2014) 1575-1587.
[9] H. Wang, G. Adluru, L. Chen, E.G. Kholmovski, N.K. Bangerter, E.V.R. DiBella, Radial simultaneous multi-slice CAIPI for ungated myocardial perfusion, Magnetic resonance imaging, 34 (2016) 1329-1336.
[10] D. Stäb, C.O. Ritter, F.A. Breuer, A.M. Weng, D. Hahn, H. Köstler, CAIPIRINHA accelerated SSFP imaging, Magnetic Resonance in Medicine, 65 (2011) 157-164.
[11] G. Adluru, C. McGann, P. Speier, E.G. Kholmovski, A. Shaaban, E.V. Dibella, Acquisition and reconstruction of undersampled radial data for myocardial perfusion magnetic resonance imaging, Journal of magnetic resonance imaging : JMRI, 29 (2009) 466-473.
[12] E.V.R. DiBella, L. Chen, M.C. Schabel, G. Adluru, C.J. McGann, Myocardial perfusion acquisition without magnetization preparation or gating, Magnetic Resonance in Medicine, 67 (2012) 609-613.
[13] B. Sharif, R. Dharmakumar, R. Arsanjani, L. Thomson, C.N. Bairey Merz, D.S. Berman, D. Li, Non–ECG-gated myocardial perfusion MRI using continuous magnetization-driven radial sampling, Magnetic Resonance in Medicine, 72 (2014) 1620-1628.
Figures