3253
Myocardial Edema Imaging using Single-shot T2STIR Prepared bSSFP1Paul C. Lauterbur Research Centre for Biomedical Imaging, Shenzhen Institutes of Advanced Technology,Chinese Academy of Sciences, Shenzhen, People's Republic of China, 2Department of Cardiology, West China Hospital, Chengdu, People's Republic of China
Synopsis
STIR-TSE is useful in imaging myocardial edema. However, it is sensitivity to cardiac motion, resulting in myocardial inhomogeneity. T2p-bSSFP overcomes this issue, but averaging is commonly used to improve its contrast. We propose a novel single-shot imaging technique that generates "STIR like" contrast and improves contrast between edema and normal myocardium compared to T2p-bSSFP. The performance of the new sequence (T2STIR-bSSFP) was evaluated by phantom study and in patients with acute myocardial infraction. The results show that the average CNR of T2STIR-bSSFP between edema and myocardium was 1.9 times better than T2p-bSSFP.
BACKGROUND
Dark blood STIR-TSE (STIR-TSE) [1] is a useful technique in imaging myocardial edema in acute myocardial infraction (MI) or myocarditis. However, this technique is sensitive to cardiac motion, leading to myocardial signal loss and hence myocardial inhomogeneity. Coil sensitivity variation further increases myocardial signal variation. T2-preparaed bSSFP (T2p-bSSFP) was proposed to overcome these issues [2]. However, averaging is commonly used to improve its contrast and thus prolongs scan time. This study proposes a new single-shot imaging technique that is insensitive to cardiac motion and shows improved contrast between edema and normal myocardium compared with T2p-bSSFP.MATERIALS and METHODS
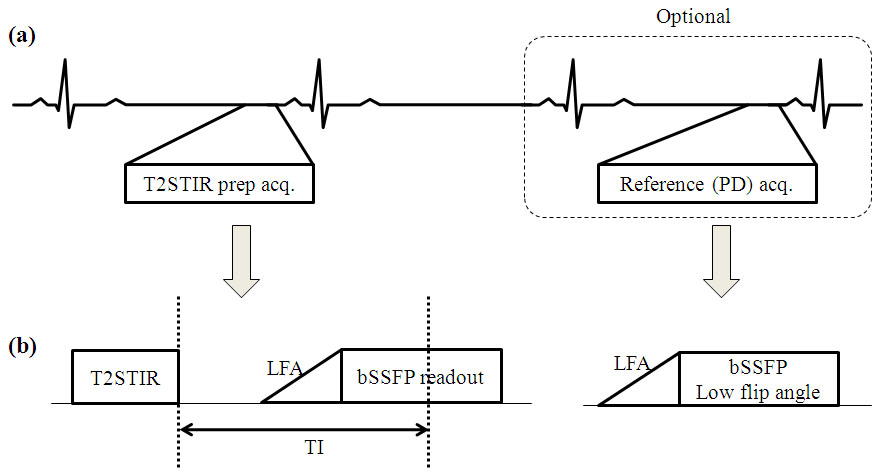
Method: Recent study found that both T1 and T2 values of edematous tissues are elevated [3]. Introducing T1 weighting to T2 preparation would increase its sensitivity to edema detection. Here, a new preparation module call “T2STIR” is used to generate “STIR like” contrast using an adiabatic pulse designed to tip the magnetization down to –z axis after T2 preparation. After the inversion time (TI) selected to null fat signal, single-shot bSSFP is then used for image acquisition. Optionally, a proton density (PD) weighted reference image is acquired in a separate heart beat for surface coil intensity correction (Figure 1). Both acquisitions are timed to mid-diastole. The sequence is referred to as T2STIR-bSSFP.
Experiment: The sequence was implemented on a 3T MR system (TIM TRIO, Siemens, Erlangen). Its performance was first evaluated in a ECV phantom (Resonance Health, Australia). The blood compartment acted as a surrogate for edema as its T1 and T2 values were both longer than the myocardium compartment. It was then evaluated in eight patients with acute myocardial infraction (IRB approved with informed consent). T2STIR-bSSFP and T2p-bSSFP images were acquired and compared. Imaging parameters: TR=2.6ms, flip angle=60o, base resolution=192, FOV=360×260mm, GRAPPA R=2, TEprep=60ms, ten linear increasing flip angle pulses (LFA) for catalyzation, linear reordering and TI=125ms for T2STIR-bSSFP. To facilitate the performance comparison with T2p-bSSFP, the same reconstruction program was used for both sequences. To clearly demonstrate the pathology, STIR-TSE, T1 and T2 maps and LGE images were also acquired to illustrate the edematous myocardium.
RESULTS AND DISCUSSION
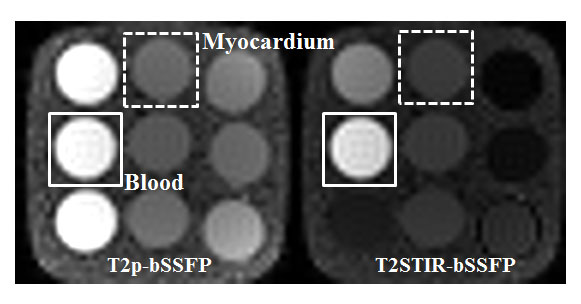
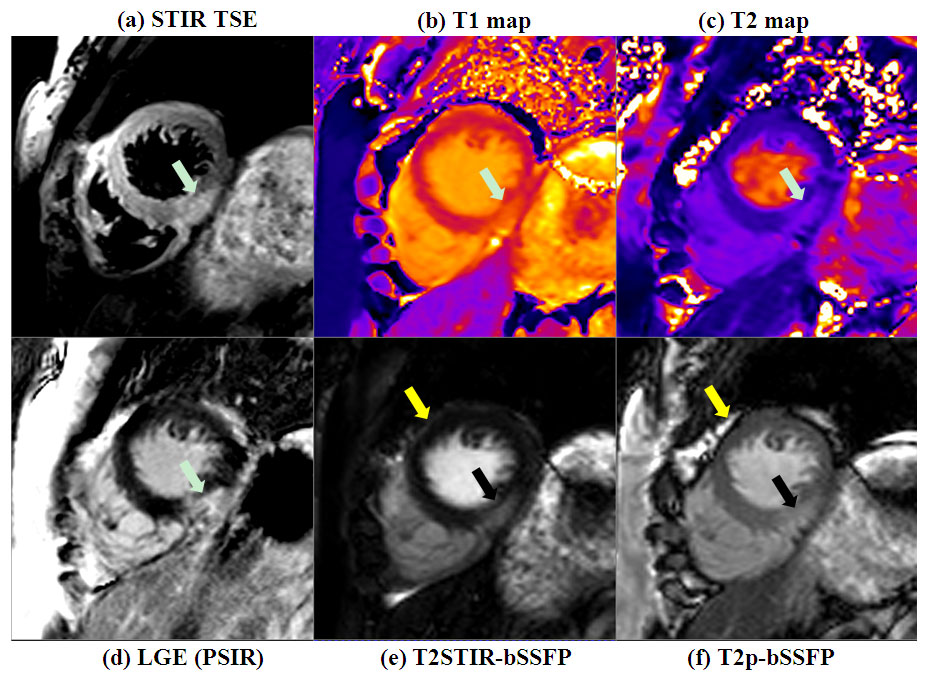
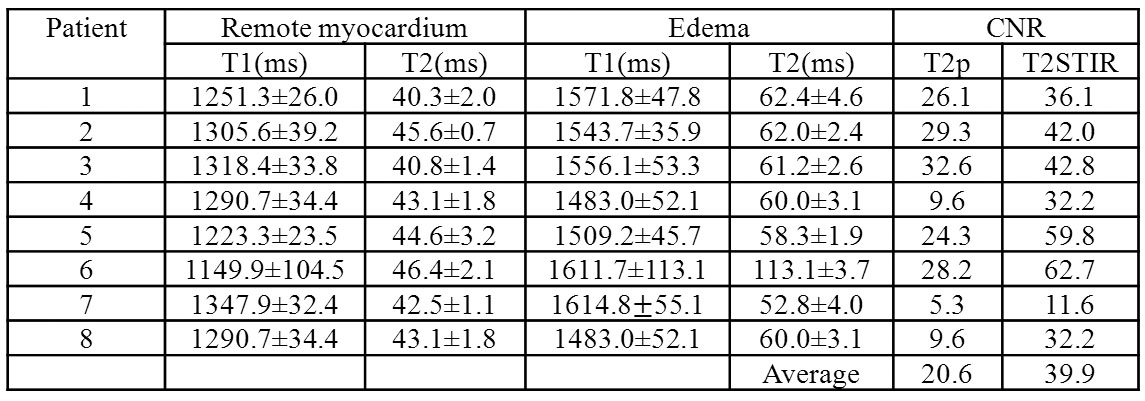
Figure 2 shows the images of the phantom using T2p-bSSFP and T2STIR-bSSFP at TEprep=60ms. The two images are windowed to the same level. The signals of the blood compartment using the two sequences are relatively similar while the signal of the myocardium compartment in T2STIR-bSSFP is significantly lower than that in T2p-bSSFP. It is been evaluated that T2STIR-bSSFP has CNR improved by 59% compared with T2p-bSSFP. Figure 3 shows the images from one patient with myocardial edema. T2STIR-bSSFP and T2p-bSSFP images are also windowed the same to facilitate comparison. Signal for remote myocardium is lower in T2STIR-bSSFP compared to T2p-bSSFP while the reverse is true for edema. Fat suppression in T2STIR-bSSFP eliminates the dark rim at the fat-water interface, and helps distinguish between pericardial fluid and fat. Table 1 shows the T1 and T2 values of myocardium and edema, and the CNRs between them in all the patients. The CNRs between edema and normal myocardium in T2STIR-bSSFP are about 1.4~3.4 times higher than T2p-bSSFP.CONCLUSION
The proposed T2STIR- bSSFP has improved contrast compared with T2p-bSSFP in myocardial edema imaging. In patient study, the average CNR of T2STIR-bSSFP between edema and myocardium was 1.9 times better than T2p-bSSFP. The proposed technique would help improve the robustness of edema imaging in cardiac patients.Acknowledgements
This work was supported by grants from the National Natural Science Foundation of China (61401449).References
1. Simonetti OP, Finn JP, White RD,et.al., "Black blood" T2-weighted inversion-recovery MR imaging of the heart. Radiology 1996;199(1):49-57.
2. Kellman P, Aletras AH, Mancini C, et.al., T2-prepared SSFP improves diagnostic confidence in edema imaging in acute myocardial infarction compared to turbo spin echo. Magn Reson Med 2007;57(5):891-897.
3. Ugander M, Bagi PS, Oki AJ,et.al., Myocardial edema as detected by pre-contrast T1 and T2 CMR delineates area at risk associated with acute myocardial infarction. JACC Cardiovasc Imaging 2012;5(6):596-603.
Figures