3242
Spiral simultaneous multi-slice first-pass myocardial perfusion imaging1Medicine, University of Virginia, Charlottesville, VA, United States, 2Biomedical Engineering, University of Virginia, Charlottesville, VA, United States, 3Radiology, University of Virginia, Charlottesville, VA, United States
Synopsis
First-pass contrast-enhanced myocardial perfusion imaging is an important tool to assess patients with coronary artery disease, but current techniques are still limited by spatial-temporal resolution and ventricular coverage. Simultaneous multi-slice (SMS) utilizes multi-band (MB) RF pulses which can greatly improve sampling efficiency. We develop an SMS-spiral perfusion pulse sequence by modulating the phase of excitation RF pulses of multiple slices with a Hadamard matrix to achieve significant signal cancellation and an incoherent aliasing pattern. The pulse sequence is evaluated in 23 patients with MB factors of 2, 3 and 4 resulting in high image quality.
Introduction
First-pass contrast-enhanced myocardial perfusion imaging is an important tool to assess patients with coronary artery disease1. However, the technique has not yet gained widespread clinical adoption due to limited spatial-temporal resolution and ventricular coverage. In our previous work, we utilized short spiral readouts and two interleaved slices per excitation to achieve whole heart coverage2. Interleaving slices increase the temporal footprint by a factor of 2, and short readouts limit the inherent SNR of the raw data. Simultaneous multi-slice (SMS) techniques3 utilizing multi-band (MB) RF pulses have the potential to significantly improve the sampling efficiency without the above limitations. Thus, the goal of this study is to utilize SMS to achieve at least 6 slices of ventricular coverage while maintaining high spatial-temporal resolution.Methods
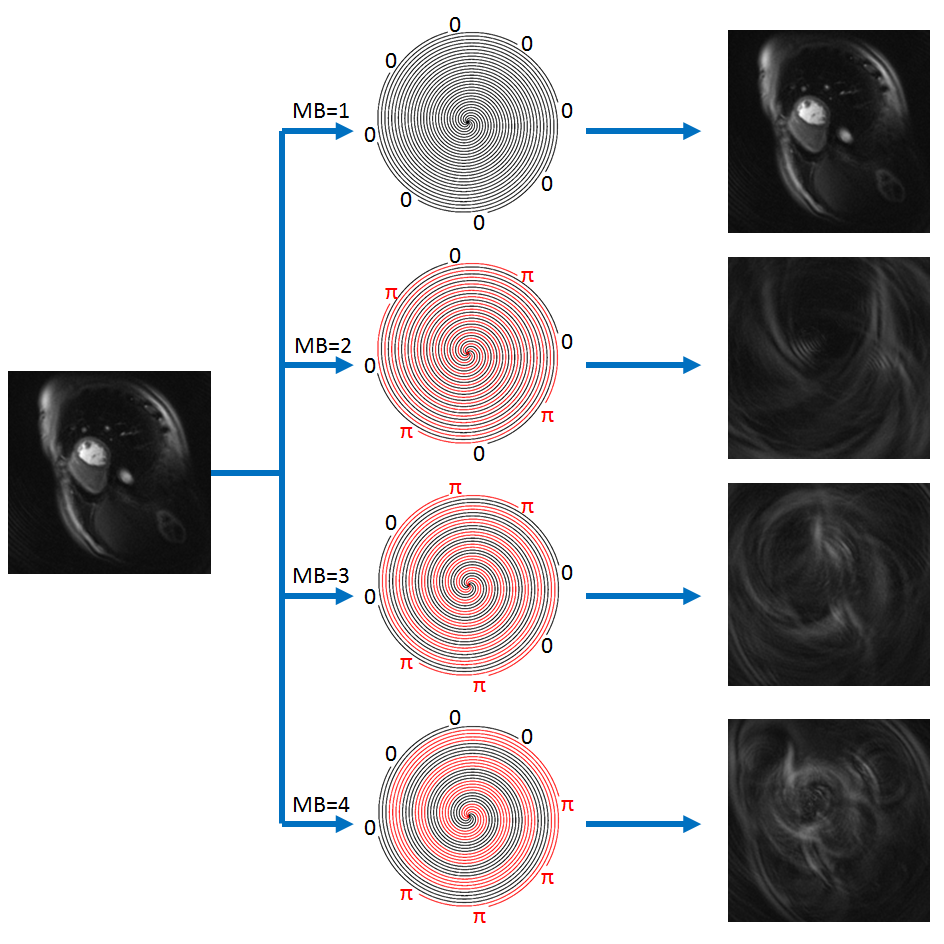
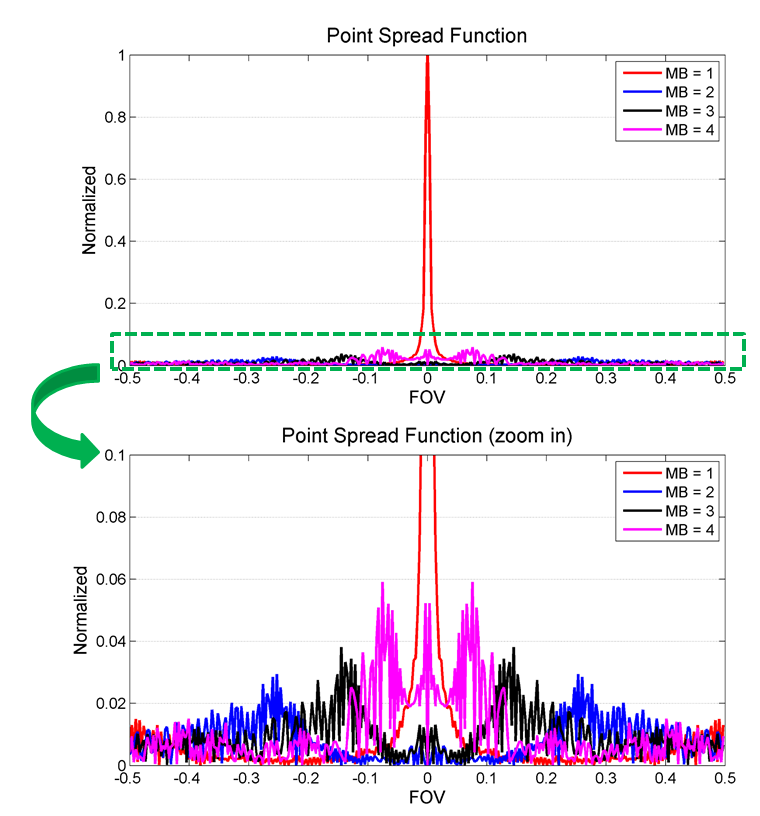
We developed an SMS-spiral perfusion pulse sequence by modulating the phase of excitation RF pulses of multiple slices by a Hadamard matrix to achieve significant signal cancellation and an incoherent aliasing pattern. Figure 1 shows an example of phase modulation of 8 spiral interleaves at MB=1 (no modulation), MB=2 ([0 $$$\pi$$$ 0 $$$\pi$$$ 0 $$$\pi$$$ 0 $$$\pi$$$]), MB=3 ([0 0 $$$\pi$$$ $$$\pi$$$ 0 0 $$$\pi$$$ $$$\pi$$$]) and MB=4 ([0 0 0 0 $$$\pi$$$ $$$\pi$$$ $$$\pi$$$ $$$\pi$$$]). We also examined the point spread function (PSF) to further validate the SMS performance (Figure 2). The excitation phase modulation was incremented by the golden-angle between heartbeats to achieve temporal incoherence. The perfusion images were reconstructed using a SMS-L1-SPIRiT technique modeling as follows:
$$\underset{x}{argmin} \lVert DF \Phi x - y \rVert^2 + \lambda_1 \lVert (G-I)x \rVert^2 + \lambda_2 \lVert \Psi x \rVert_1$$
Where $$$F$$$ is a Fourier operator which transfers the data from image domain to k-space domain, $$$D$$$ is the inverse gridding operator that transfers the Cartesian grid to a spiral trajectory, $$$G$$$ is an image-space SPIRiT operator that represents the k-space self-consistency convolutions in the image domain, $$$\Psi$$$ is the finite time difference transform that operates on each individual coil separately to achieve sparsity in the temporal domain of image time series, and $$$\Phi$$$ combines the multiple phase modulation slices to a single SMS slice. $$$\lambda_1$$$ and $$$\lambda_2$$$ balance the data acquisition consistency with calibration consistency and sparsity. The calibration kernel is derived from an upfront scan without SMS acquisition. We included 23 patients undergoing clinically ordered CMR studies with gadolinium on a 1.5T Aera Siemens scanner in this study. 10 studies were performed at MB=2, 10 studies were performed at MB=3, and 3 were performed at MB=4. Other sequence parameters included: FOV 340mm, TE 1.0ms, TR 8ms, SRT 80ms, FA 26o, 6 to 9 slices with 10mm thickness, 2mm in-plane resolution. 3 slices were selected from all patient perfusion images to be blindly graded on a 5-point scale (5 = excellent, 1 = poor) by a cardiologist for image quality assessment.
Results
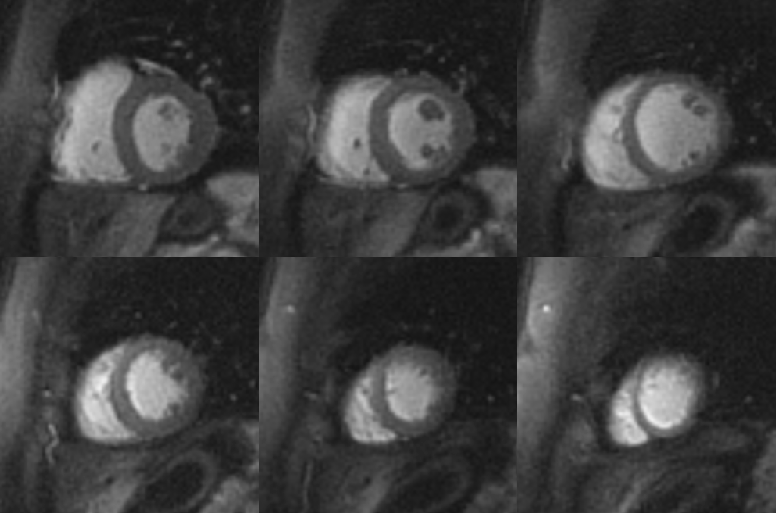
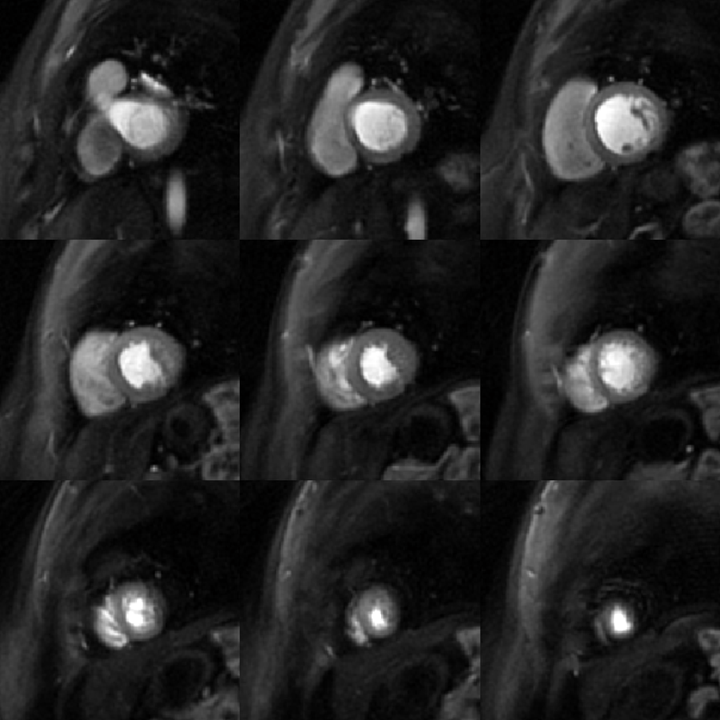
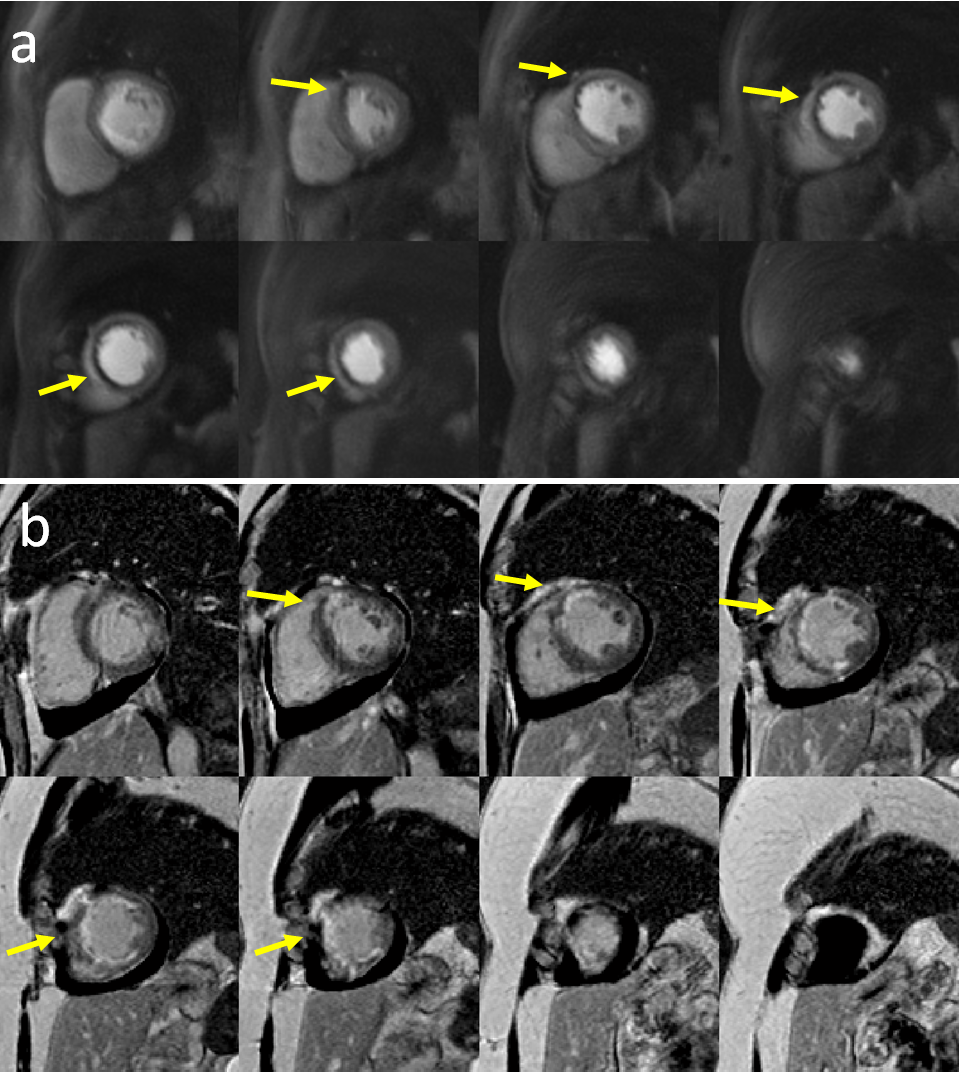
Figure 2 shows the PSF of the MB=1, and the interference pattern added by the additional excited slices for an MB=4 acquisition. The main lobe energy was cancelled for MB 2, 3 and 4, and the side lobe amplitudes were 6% of MB1 main lobe amplitude with an incoherent pattern suitable for SMS-L1-SPIRiT reconstruction. Figure 3 presents an acquisition with an MB factor of 2 with 6 slices per heartbeat. Figure 4 shows an example case acquired with an MB factor of 3 with 9 slices per heartbeat. Both cases result in high image quality while maintaining the same spatial-temporal resolution. Figure 5 demonstrates perfusion images from a ST-elevation myocardial infarction (STEMI) patient at a MB factor of 4. Even at a higher MB factor, the images (a) clearly delineate a perfusion abnormality with a location corresponding to the infarction on the LGE images (b). The image quality scores were 3.95±0.68 (MB=2), 4.05±0.89 (MB=3) and 4.5±0.5 (MB=4), with no significant quality difference in image quality between MB factors (p=0.40).Conclusion
We demonstrated the successful application of an SMS spiral perfusion at MB factors of 2, 3 and 4. Due to the increased sampling efficiency of SMS, whole heart coverage is achieved with high image quality without the need for interleaving slices or significantly shortening readout time. Further validation will be required in patients undergoing adenosine stress CMR.Acknowledgements
This work was supported by NIH K23 HL112910 and 5T32EB003841.References
1. Nagel E, Klein C, Paetsch I, Hettwer S, Schnackenburg B, Wegscheider K, Fleck E. Magnetic resonance perfusion measurements for the noninvasive detection of coronary artery disease. Circulation 2003;108(4):432-7.
2. Yang Y, Kramer CM, Shaw PW, Meyer CH, Salerno M. First-pass myocardial perfusion imaging with whole-heart coverage using L1-SPIRiT accelerated variable density spiral trajectories. Magn Reson Med 2015.
3. Barth M, Breuer F, Koopmans PJ, Norris DG, Poser BA. Simultaneous multislice (SMS) imaging techniques. Magn Reson Med 2016;75(1):63-81.
Figures