3236
Coronary flow velocity reserve by 3T-MRI fast velocity-encoded cine can detect patients with high-risk coronary artery disease1Hokkaido University Graduate School of Medicine, Sapporo, Japan
Synopsis
Low coronary flow velocity reserve (CFVR) on left main coronary trunk can predict downstream coronary organic stenosis and myocardial scar, suggesting that CFVR derived by flow velocity by MRI is a simple and reliable index to detect patients with high-risk coronary artery disease.
Purpose
The effects of coronary stenosis on downstream flow reserve have been well established.1, 2 However, there is technical limitation to measure flow velocity on distal vessels by noninvasive modality.3 We have developed a reliable method to estimate coronary flow velocity reserve (CFVR) in the left main trunk artery (LM) as an index of entire coronary circulatory function by using velocity-encoded cine 3-tesla magnetic resonance imaging (MRI). The purpose of our study was to evaluate whether the CFVR in LM can predict downstream atherosclerotic burden in the left anterior descending artery (LAD) and left circumflex artery (LCX).
Methods
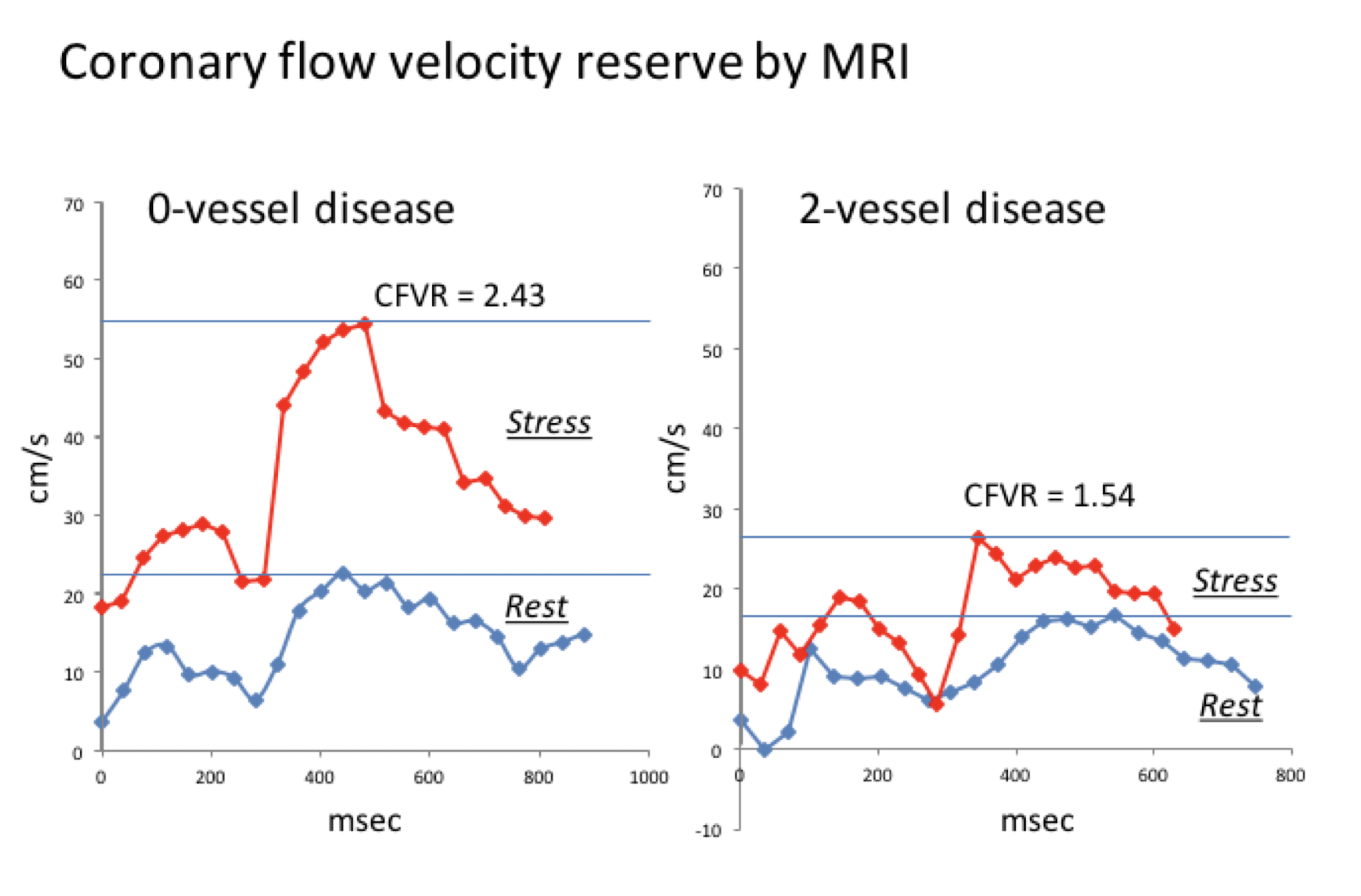
Consecutive 35 patients with coronary artery disease (CAD) who underwent both invasive coronary angiography and MRI (age; 68 ± 8 yr, male; n=18) and 16 healthy male volunteers (age; 28 ± 8 yr) were studied. CFVR in LM was measured with breath-hold velocity-encoded cine 3-Tesla MRI during adenosine triphosphate stress and at rest. CFVR was calculated by dividing peak-velocity during stress by that at rest (Figure 1). Myocardial scar was evaluated by late gadolinium enhancement. Per-patient angiographic disease burden in the LM, LAD, and LCX were scored with the use of the Leaman score (LS).4Results
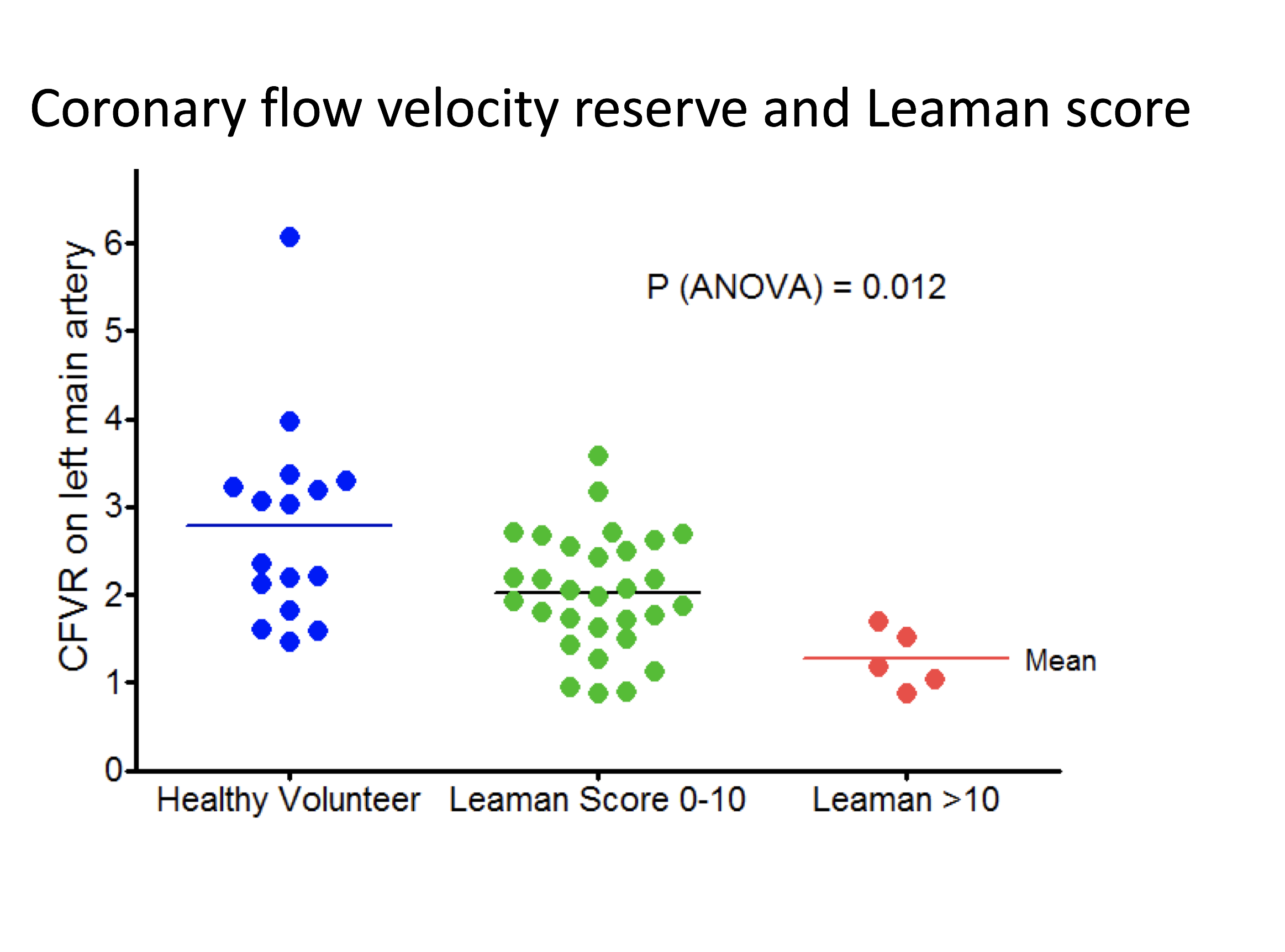
Thirty of 35 patients had low LS (0-10) and 5 had high LS (≧10.5, equivalent to ≧90% stenosis in a proximal LAD). CFVR with high LS patients was significantly lower than that with low LS patients and healthy volunteers (Figure 2). Likewise, CFVR in patients with late gadolinium enhancement (LGE) (n = 9) was significantly lower than that with negative LGE (1.38 ± 0.46 vs. 2.11 ± 0.65, P < 0.05). The receiver operator curve showed the high discrimination for high-risk CAD by CFVR of less than 1.70 (area under curve = 0.89) with the sensitivity of 100% and the specificity of 76%.Conclusion
Low CFVR derived by flow velocity by MRI on LM can predict downstream coronary organic stenosis and myocardial scar, suggesting that CFVR is a simple and reliable index to detect patients with high-risk CAD.Acknowledgements
NoneReferences
1. Naya M, Murthy VL, Blankstein R, Sitek A, Hainer J, Foster C, et al. Quantitative relationship between the extent and morphology of coronary atherosclerotic plaque and downstream myocardial perfusion. J Am Coll Cardiol 2011;58:1807-1816.
2. Taqueti VR, Hachamovitch R, Murthy VL, Naya M, Foster CR, Hainer J, et al. Global coronary flow reserve is associated with adverse cardiovascular events independently of luminal angiographic severity and modifies the effect of early revascularization. Circulation 2015;131:19-27.
3. Sakuma H, Koskenvuo JW, Niemi P, Kawada N, Toikka JO, Knuuti J, et al. Assessment of coronary flow reserve using fast velocity-encoded cine MR imaging: validation study using positron emission tomography. AJR Am J Roentgenol 2000;175:1029-1033.
4. Leaman DM, Brower RW, Meester GT, Serruys P, van den Brand M. Coronary artery atherosclerosis: severity of the disease, severity of angina pectoris and compromised left ventricular function. Circulation 1981;63:285-299.
Figures