3235
The importance of correcting for through-plane heart motion in the assessment of aortic regurgitation using PC-MRI as estimated by feature tracking cine-MRIFrida Svensson1,2, Alexander Johansson3, Åse Johnsson2,3, and Kerstin Magdalena Lagerstrand1,2
1Dept. of Medical Physics and Techniques, Sahlgrenska University Hospital, Gothenburg, Sweden, Sahlgrenska University Hospital, Gothenburg, Sweden, 2Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden, 3Dept of Radiology, Sahlgrenska University Hospital, Gothenburg, Sweden, Sahlgrenska University Hospital
Synopsis
Phase contrast measurements are prone to velocity offsets due to through-plane motion of the heart. Here we examine the impact of these velocity offsets on the assessment of aortic regurgitation using a promising method for quantification of the through-plane heart motion. Without correction for through-plane heart motion, the phase contrast measurements significantly underestimated the severity of the regurgitation and the underestimation varied highly between individuals. This calls for development of reliable and robust methods, such as the proposed tracking method, for individual correction of through-plane heart motion in the phase contrast measurements.
Purpose
Assessment of the severity of aortic regurgitation (AR) with phase contrast (PC) MRI rely on the quantification of regurgitation volumes (RV) and fractions (RF). However, PC measurements are prone to velocity offsets due to through-plane motion of the heart, leading to underestimation of RV and RF [1]. Such underestimation may have a clinical impact on the assessment of the AR severity and may consequently cause a delay in patient treatment. This work aims to investigate the impact of through-plane heart motion on the assessment of AR, utilizing a novel feature tracking method for quantification of the through-plane heart motion.Methods
Thirty-four AR patients with various severity and aortic dimensions were examined with cardiac MRI on a 1.5T scanner (Achieva, Philips Healthcare, Best, The Netherlands). The examination protocol included 2D PC MRI at the ST-junction (FOV=320x260mm2, voxel=2.5x2.5mm2, slice=6mm, flip=12°, TR=4.8ms, TE=2.9ms, frames=40, acc=2), but also conventional cine-MRI in SA- and LA-views (FOV=320x260mm, voxel=1.7x1.7mm, slice=8mm, flip=60°, TR=3.4ms, TE=1.7ms, frames=30, acc=2) . From the PC measurements, estimates of RV and RF were derived. Through-plane-heart-velocity-time-curves and estimates of peak heart velocity at systole and diastole were also derived using feature tracking cine-MRI (described in detail in a separate abstract “The feasibility of correcting for the effect of through-plane heart motion on phase contrast aortic blood flow measurements using feature tracking cine-MRI”). Data corrected for through-plane heart motion were compared with uncorrected data, where differences at p<0.05 was considered significant.Results
Without correction for through-plane heart motion, the PC measurements displayed smaller values of RV (12±5 ml) and RF (5±3%) that led to a lower grading of the AR severity in 24% of the patients (Figure 1). The magnitude of the underestimation varied between individuals and depended strongly on the peak heart velocity and the aortic dimension (p<0.001; Figure 2). As expected, the relative effect of through-plane heart motion on the quantification of RV and RF was largest for patients with mild and moderate AR, but was significant also for patients with severe AR (Table 1). For RF, the absolute error also increased significantly with decreased AR severity (Table 1).Discussion
This work shows that through-plane heart motion impacts the assessment of AR using PC MRI. After correction, a number of individuals were categorized as having a more severe AR. Hence, one may expect that a number of AR patients could be erroneously diagnosed regarding the grading of the AR severity if through-plane heart motion correction of the PC measurements is not applied. The work also demonstrates the importance of individual correction of through-plane heart motion in the assessment of AR using PC-MRI. The underestimation of RV and RF varied highly between individuals, mainly due to large differences in the aortic dimension and peak heart velocity. It should be pointed out that the effect of heart motion is not only a problem for blood flow measurements based on 2D PC MRI, but also for 4D Flow. Similarly as for the 2D image slice, the 3D image volume is fixed in space causing the heart to move through the volume during scanning and thereby adding velocity offsets to the blood flow data.Conclusion
The assessment of AR using PCI-MRI is significantly affected by through-plane heart motion. The effect varies depending on aortic dimension and through-plane heart velocity. This calls for development of methods for individual correction of through-plane heart motion. In this work we utilize a promising method based on the inherent information of the cardiac MRI examination. Further studies are warranted to investigate whether such through-plane valvular motion correction can improve patient management.Acknowledgements
No acknowledgement found.References
1. Kozerke S, Schwitter J, Pederson E, Boesiger P. Aortic and Mitral Regurgitation: Quantification Using Moving Slice Velocity Mapping. JMRI 14:106–112 (2001).Figures
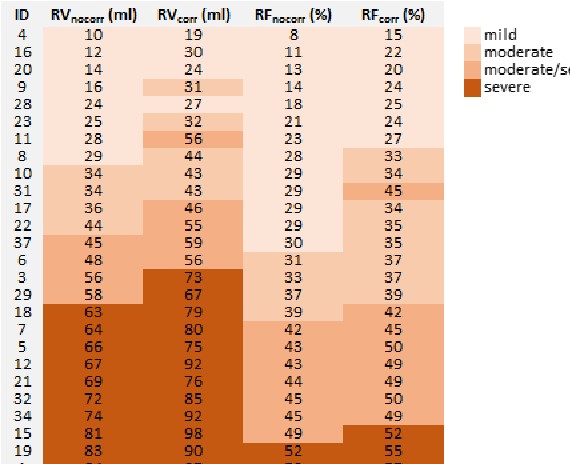
Figure
1. The grading of AR severity in all individuals based on values of
regurgitation volume (RV) and fraction (RF), uncorrected and corrected for
through-plane heart motion.
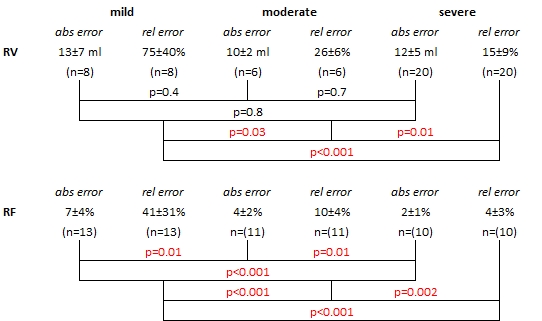
Table 1. Absolute and relative errors in the
regurgitation volume (RV) and fraction (RF) due to through-plane heart motion. Significant
differences between groups of patients with different grades of severity is a
marked with red.

Figure
2. The relation between the flow volume error during systole and diastolic and the
aortic area (a-b) or the systolic and diastolic peak heart velocity (c-d).