3230
Improving visualization of cardiac QFlow by acquiring bSSFP cine images within the same breath holdMatthew Lanier1, Ryan Moore2, Michael Taylor2, Charles Dumoulin1, and Hui Wang3
1Radiology, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States, 2Cardiology, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States, 3Philips, Cincinnati, OH, United States
Synopsis
In this study, we propose a method to acquire QFlow and bSSFP cine images in a single breath-hold that eliminates the need to have these scans acquired separately; thereby overcoming the need for inter-breath hold cross-registration. The approach provides improved registration of flow fields with high-resolution anatomic cine imaging.
Introduction
Cardiac phase-contrast MRI (PC-MRI) is a non-invasive method for evaluating cardiopulmonary hemodynamics (ref 1, 2). Clinically, the most common cardiac PC-MRI acquisition is applied through the ascending and descending aorta for measuring cardiac output. However, since PC-MRI is a spoiled gradient echo sequence, the delineation of the vessel wall can be poor, when compared to a bSSFP sequence. In order to better visualize flow near the vessel wall, QFlow and bSSFP cine on the same plane are acquired sequentially in two separate breath holds (BH) as shown in Fig 1. In this study, we propose a novel acquisition strategy in which both QFlow and bSSFP cine images are acquired within the same breath hold.Materials and Methods
The combined acquisition protocol was achieved by employing a dedicated MR system architecture that enables “Multiple Instantaneous Switching between Scans” (or MISS) (ref 3 and 4), which allows for interleaved QFlow and bSSFP cine acquisitions within the same breath-hold (Fig 2). Volunteer imaging was performed at 1.5T Ingenia™ scanner (Philips, Best, Netherlands) using posterior and anterior phased array coils for signal reception. Cardiac synchronization was achieved with vector cardiographic (VCG) gating. Seven healthy volunteers were imaged for this feasibility study. For the QFlow sequence, the scan parameters were as follows: TR=4.1ms; TE=2.5ms; FA=12°; FOV=200-300x200-300mm, in plane resolution=2.5x2.5mm, slice thickness=8mm; SENSE factor=2, VENC=200cm/s. For the bSSFP cine sequence, the scan parameters were as follows: TR=2.4-2.7ms; TE=1.2-1.4ms; FA=60°; FOV = 200-300x200-300mm, in plane resolution 2x2mm, slice thickness=6mm; SENSE factor=2. Both sequences used retrospective triggering and 30 cardiac phases were reconstructed. This ensured temporal alignment between the two sequences. In this feasibility study, a clinical acquisition protocol with an imaging plane across the ascending and descending aorta was used. bSSFP cine was acquired first over a period of 3-5 seconds, followed by the QFlow sequence which took about 10 seconds. The entire breath hold was 13-15 seconds long.Results
In all subjects, the combined QFlow and bSSFP cine approaches were acquired successfully. The approach not only provided half as many BHs from n=2 (1xcine+1xQFlow) to n=1 combined BHs, but also kept the geometry exactly the same since there was no inter-BH motion. The prep times per BH doubled due to the application of both bSSFP cine and QFlow prescans. However, conventional cross-registration steps were eliminated by the single-BH QFlow and bSSFP cine scheme. In the acquired planes, no extensive registration beyond in-plane resolution was required. Since bSSFP cine and QFlow are set to the same number of cardiac phases, no phase adjustments were needed. The contours of the ascending and descending aorta from bSSFP cine could be directly used in QFlow analysis. Fig. 3 shows QFlow and bSSFP cine images acquired with the proposed technique. The contrast between blood and vessel wall in bSSFP cine images is improved, compared with QFlow magnitude images, especially in the diastolic phases.Conclusion
We have demonstrated the feasibility of a combined single-BH acquisition of flow and cine sequences improving the visualization of vessel walls and contour accuracy. The technique eliminates inter-BH motion and the need for post-processing image registration between bSSFP cine images and QFlow images. This acquisition approach provides a clinically translatable cardiac flow assessment that inherently prevents inter-scan motion, and requires fewer breath-holds per exam. The next step is to further optimize the protocol to shorten breath hold times and apply this technique on patients. This could be applied to pulmonary artery and other vessel planes as well.Acknowledgements
We would like to thank Jouke Smink and David Higgins of Philips for providing technical advice.References
[1] - Lotz et al. Radiographics 2002, 22(3):651-71. [2] - Gatehouse et al. Eur Radiology 2005, 15:2172-84. [3] - Henningsson et al. MRM 2015, 73(2):692-6. [4] - Kawaji et al. SCMR 2017Figures

Figure 1. Current
clinical workflow of acquiring QFlow and bSSFP Cine consecutively in two
separate breath holds. With conventional protocol, each preparation scan must
precede each scan.
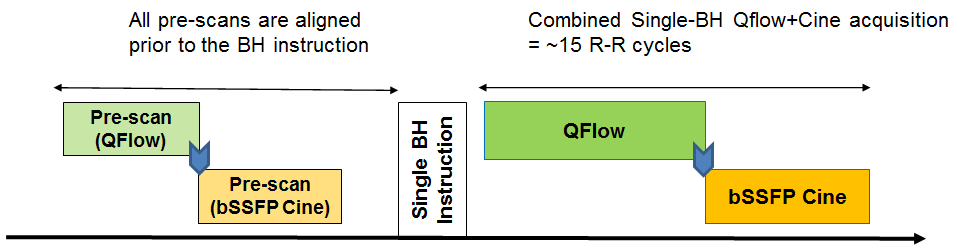
Figure 2. Proposed
workflow of combining of QFlow and bSSFP cine in a single-breath hold. The
proposed protocol permutes the preparation scan and actual scans. Using MISS
technique, after finishing QFlow scan, it instantaneously switches to bSSFP cine
scan without pause. This makes it possible to fit two different scans into one
single breath hold.
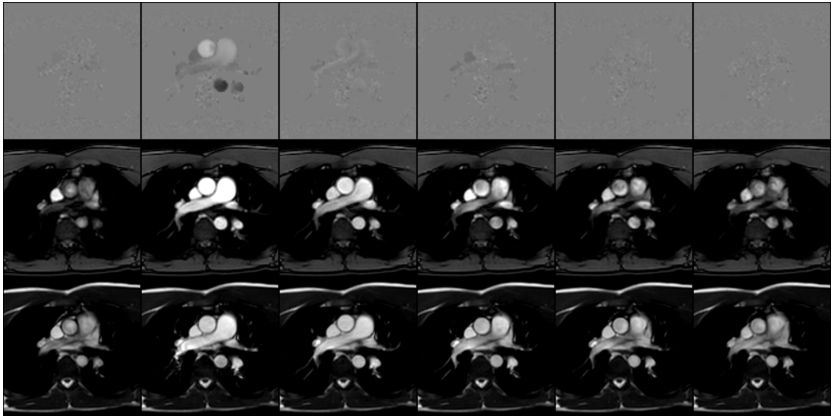
Figure 3. QFlow
and bSSFP cine images acquired with the proposed technique. Thirty frames are down-sampled to 6 frames for display
purpose. Top row shows QFlow phase images, middle row shows QFlow magnitude
images, bottom row shows bSSFP cine images. The contrast between blood and
vessel wall in bSSFP cine images is much better, comparing to QFlow magnitude
images.