3228
Combining Phase Information from Phased Array Coils without Phase Unwrapping in Phase Contrast Imaging1Alltech Medical Systems America, Solon, OH, United States, 2Alltech Medical Systems, Chengdu, People's Republic of China
Synopsis
In phase contrast flow quantitation, high spatial/temporal resolution and parallel imaging often entail the high density multiple phased array receive coils. To overcome ambiguities in coil signal combination introduced by motion, phase wrapping, image noise, and the unknown phase-offset among the coils, we used the k-space complex division of the same coil element signals from both flow compensated (FC) and flow encoded (FE) scans to eliminate the coil sensitivity phase associated with that coil element and then add all phase difference of each elements in complex domain to avoid phase unwrapping for a fast and accurate flow velocity mapping.
Purpose:
In cine phase contrast imaging technique, the image phase has been used to quantify blood flow within vessel lumen and over cardiac phases. High spatial/temporal resolution and parallel imaging often entail the high density multiple phased array receive coils. However, accurate combining MR phase information from them is complicated by ambiguities introduced by motion, phase wrapping, image noise, and the unknown phase-offset among the coil elements [1]. Various techniques require additional reference scans and/or offline post-processing[2]. We used the k-space complex division of the same coil element signals from both flow compensated (FC) and flow encoded (FE) scans to eliminate the coil sensitivity phase associated with that coil element and then add all phase difference of each elements in complex domain to avoid phase unwrapping for a fast and accurate flow velocity mapping.Theory and Methods:
The phase estimation problem has been studies[3] and is formulated as: Phase of each channel = magnetized phase + receiver phase sensitivity. To get rid of phase from receiver sensitivity, we use complex division of the FC and FE for each channel. The phase difference (Δθ) of the complex signal of SFC and SFE (assuming SFC and SFE corresponding the FC and FE image) for the i element of coil can be calculated by the equation below. Finally, the summation over all coil elements (i) in the complex domain for our combined phase image.
Δθ = angle(Σ SFC ×conj(SFE))
Through-plane phase contrast imaging with ECG gating was acquired at the magnet iso-center on a 1.5T with 15 coils elements from both the spine coils and mid torso flex coils (Alltech Medical System, Solon, OH). The sequence parameters as follows: FOV=270 mm x 360 mm, Slice Thickness 6 mm, TE 4.8 ms, TR 9.7 ms, flip angle 20°, VENC 70 cm/s with FC and FE acquisition interleaved. Same sequence was applied to both phantom and volunteers (with written consent from the local IRB) with breath holding for ascending and descending aorta in axial plane at the pulmonary artery position. The cross-sectional views of the ascending aorta and main PA were obtained using double oblique reference images.
Results:
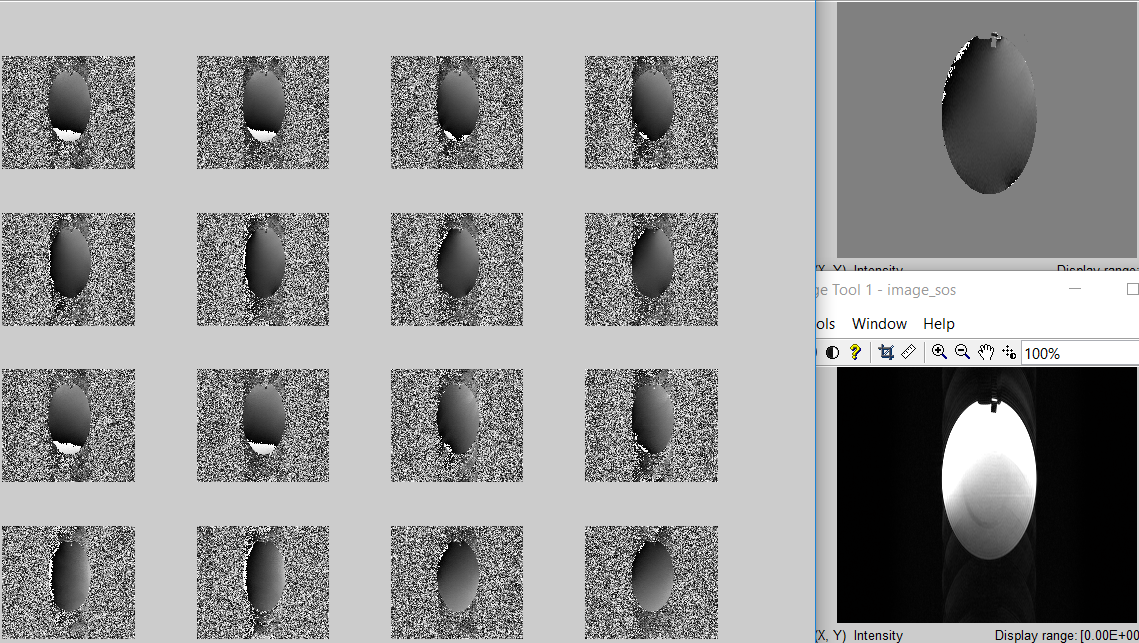
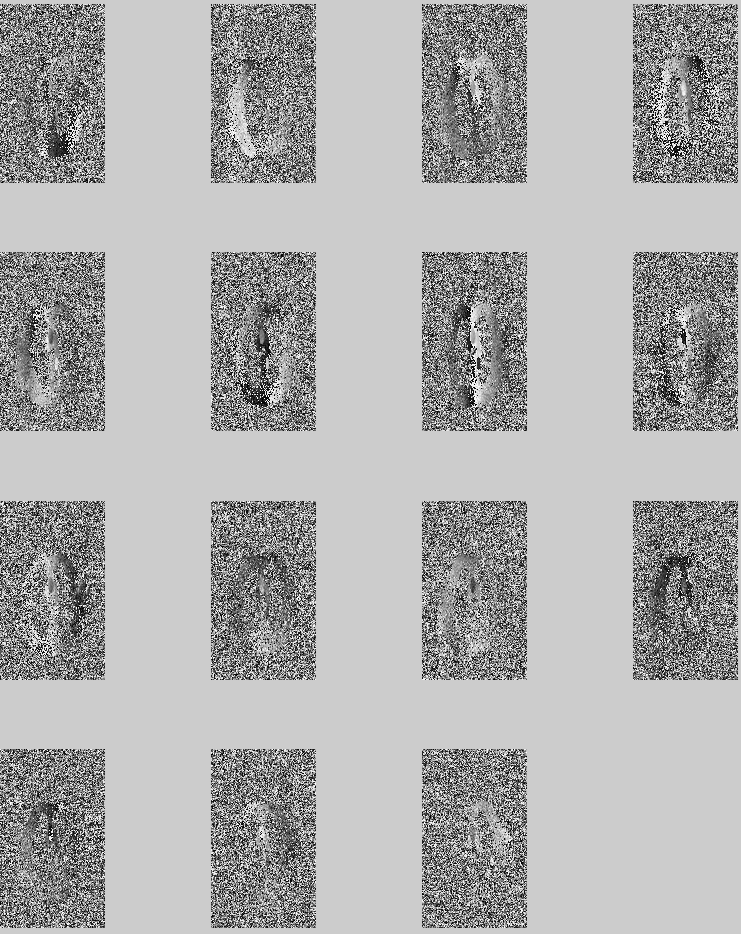
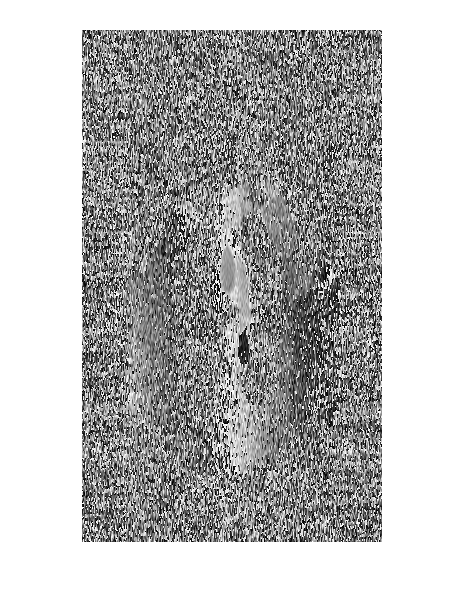
Phase combination example of phantom shows on Figure 1. The upper panel of 8 phase difference images between FC and FE scans are individual coil elements; while lower panel of 8 phase combined images demonstrates the step by step process of add phase from all the coil elements up; the resulting magnitude and phase are shown on the right. Figure 2 shows the volunteer study phase difference images for all 15 coil elements. Figure 3 shows the phase combined image from the complex summation of all channels. The aortic flow information is preserved after the phase combination.
Our proposed phase combining algorithm achieves substantial improvements in the phase estimate. The phantom and volunteer studies showed it’s a fast and reliable approach.
Conclusion and Discussion:
We developed a k-space phase combination method for phase contrast imaging, providing a potential improvement for the applications of accurate flow assessment with high density phase array coils and for clinical applications in areas with low SNR, or motion or susceptibility artifacts.
Our phase reconstruction is based on the phase difference information of FC and FE scans out of the same coil element. As a result, although the SNR at the blood vessel is great, the SNR at stationary tissue may suffer. Although this should not affect the flow quantitation, we still plan to investigate further on algorithms to provide optimal SNR over the entire phase image, as well as the magnitude.
Acknowledgements
No acknowledgement found.References
1. Robinson, S. and J. Jovicich, B0 mapping with multi-channel RF coils at high field. Magn Reson Med, 2011. 66(4): p. 976-88.
2. Parker, D.L., et al., Phase reconstruction from multiple coil data using a virtual reference coil. Magn Reson Med, 2014. 72(2): p. 563-9.
3. Bernstein, M.A., et al., Reconstructions of phase contrast, phased array multicoil data. Magn Reson Med, 1994. 32(3): p. 330-4.
Figures