3216
An MRI Phantom Study to Assess the Effects of Localized Stiffness on Aortic Hemodynamics1Laboratoire d'Imagerie par Résonance Magnétique Médicale et Multi-Modalités (IR4M), Univ. Paris-Sud, CNRS, Université Paris-Saclay, Orsay, France
Synopsis
Cardiovascular complications have been highly associated with arterial stiffness which results from aging and/or vascular disease. Reduced arterial elasticity, particularly at the aorta level, increases the left ventricle load. In this work, we studied the effects of localized stiffness on an aortic phantom with respect to its severity and position relative to an upstream proximal site. As expected, our results showed that the aortic hemodynamics were altered: the pulse pressure was increased, and the flow rate decreased. Moreover, the local proximal compliance was reduced as the stiffness was brought closer to the heart. However, the pulse wave velocity remained unchanged suggesting that global stiffness measuring approaches might not detect regional wall alterations
Introduction
The large arteries play two main functions in the systemic circulation: a "Windkessel" function and a conduit function with low resistance to blood flow. Both tasks are altered by arterial stiffness that emerges nowadays as a major risk factor. Indeed, natural aging is associated with a systemic reduction of arterial elasticity. However, localized aortic stiffness resulting from compliance-unmatched vascular prostheses and/or local wall damage also leads to cardiovascular events. While age-related stiffness effects have already been studied 1, our objective is to evaluate the effects of locally reduced compliance on arterial hemodynamics using a realistic aorta phantom. Depending on stiffness site and severity with respect to the heart, different outcomes may be observed. Such exploration can be achieved using cardiovascular Magnetic Resonance Imaging (MRI) that allows not only a non-invasive estimate of flow rates but also the assessment of the aortic distension over a cardiac cycle.Material and Methods
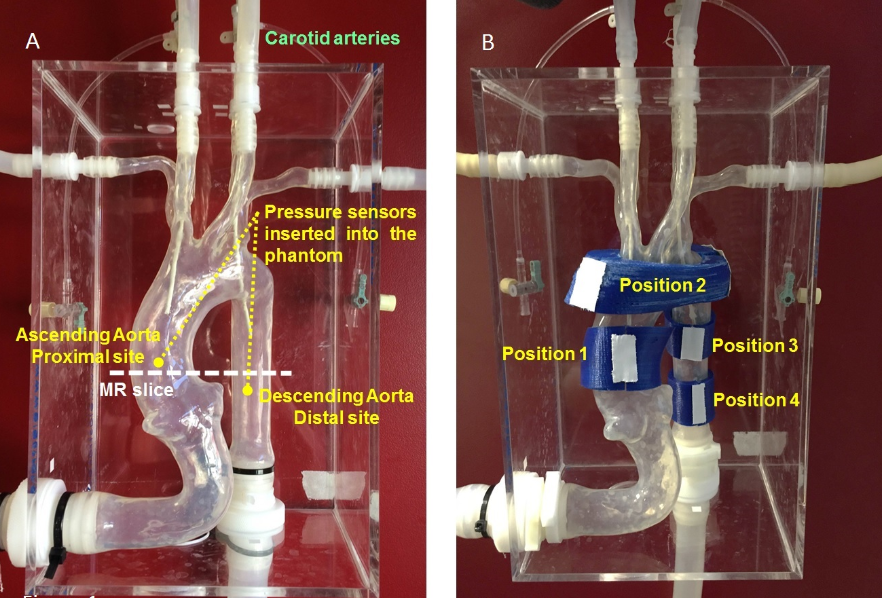
The MR-experimental setup consist of an MR-compatible pump that delivers a programmable pulsatile flow. Blood mimicking fluid was pumped in a silicone aorta phantom with realistic dimensions (Fig.1A). The aorta model was placed in the magnet of a 1.5 T Philips Achieva MRI. Localized stiffness was induced at the ascending Aorta (AA), the Aortic arch and the descending Aorta by printing 3D well-adapted rigid prints (Fig.1B) slipped around the aortic segments, thus preserving their geometry. Eight stiffness configurations were chosen: position 1 (Pos.1), Pos.2, Pos.3, Pos.4, Pos.12 (both Pos.1 and Pos.2 are stiffened), Pos.13, Pos.23 and Pos.123. MR Phase-Contrast images were acquired to quantify proximal flow while distension was assessed using Cine acquisitions under ARTFUN segmentation software 2. Pressure waves were measured using fiber optic pressure sensors inserted at a proximal and distal site. Additionally, we determined the local proximal compliance using Pressure-Area loops. Characteristic impedance (Zc) was derived from pressure and flow waveforms. Pulse wave velocity (PWV) was also calculated based on proximal-distal pressure transit time.Results
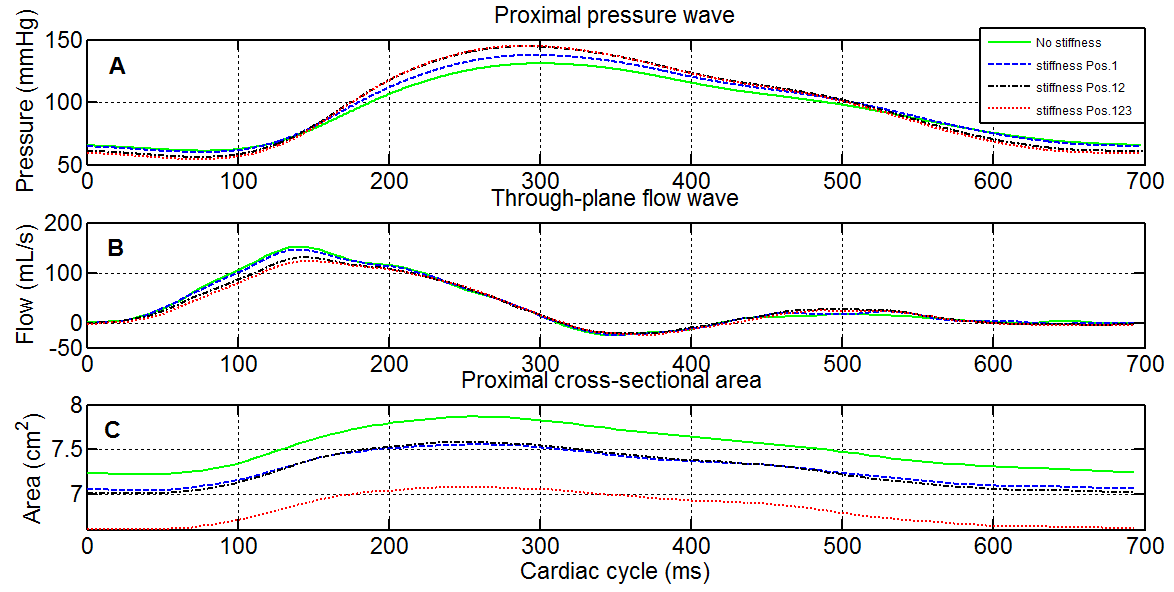
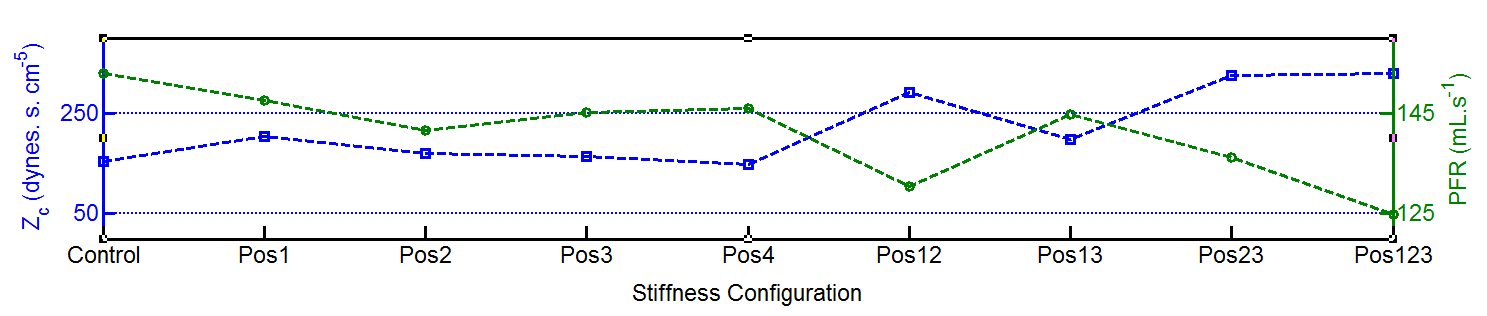
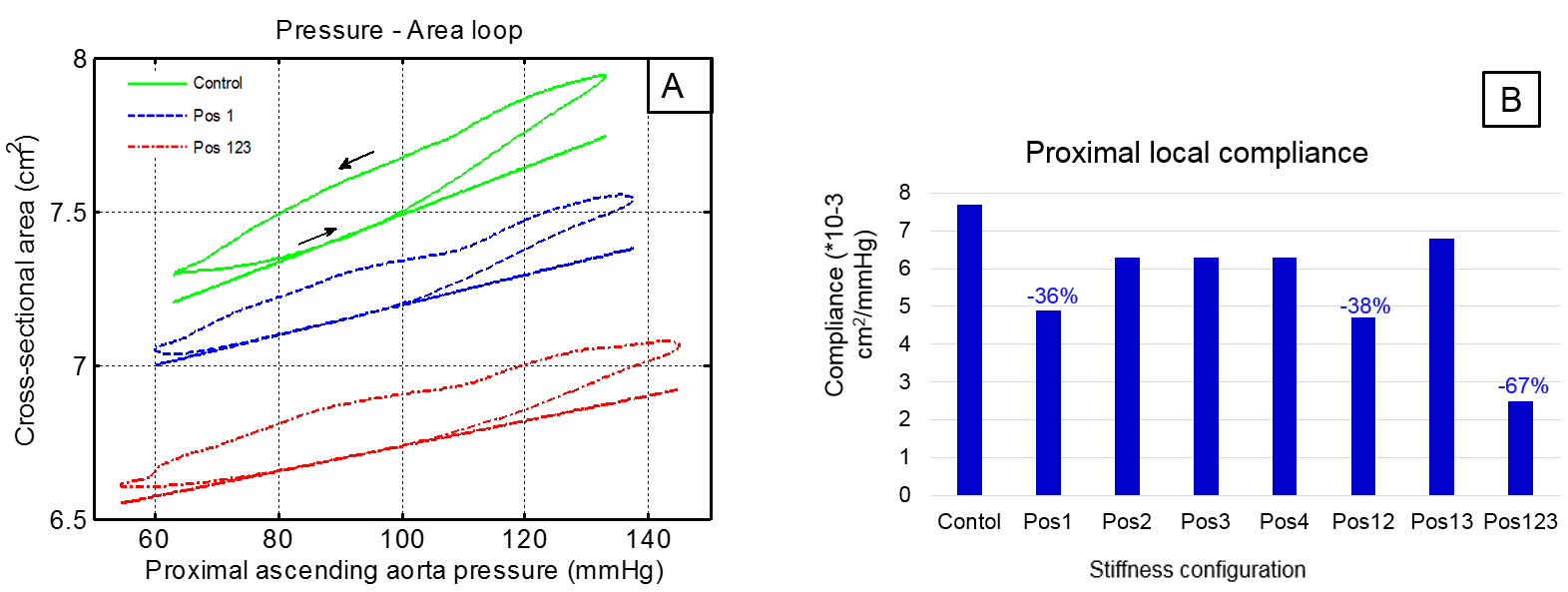
Example of proximal pressure, flow and cross-sectional area waveforms are shown in figure 2 (A, B and C respectively). The proximal pulse pressure (PPP) was increased (Fig.3) and the proximal MR-averaged flow rate underwent a drop in peak systolic value (Fig.4) regardless of the stiffened site. Considering the single stiffness configuration: stiffening the AA (Pos.1) mainly increase the PPP by 11.3% compared to the control case. Moreover, Zc was mostly increased (31%) at this position. Unlike what was observed on PP, the peak flow rate (PFR) decrease caused by the Pos2 stiffness was slightly more noticeable. Cross-sectional area was shifted to lower levels. Furthermore, proximal compliance was altered and was mostly reduced by 36% for Pos.1 (Fig.5). Accounting for multiple stiffness configuration, PP reached a maximum with a 29.7% augmentation when the stiffening occurs at Pos.123. Additionally, the effect of Pos.12 stiffness on PP seems to be quite similar to that of Pos.123. The same PP tendency was observed at the distal site. Proximal Zc is augmented by 109% in Pos.123, thus the highest drop of the PFR (-20%). The highest decrease of the proximal distensibility was observed in Pos.123 where the compliance was reduced by 48% relative to the control case. However, PWV remained unchanged with insignificant changes of the pulse transit time (3.42 ± 0.19 ms) for all stiffness casesDiscussion
Our findings indicate that a local stiffness will extend its effects centrally toward the heart. It acts by altering the pressure-area relationship as the wall displacement was reduced when wider PP is recorded. This suggests that the presence of local stiffness degrades not only local mechanical properties of the wall, but its effects extend to adjacent sites. This is in line with previously reported results 3. Indeed, local stiffness effects are more pronounced when longer parts of the aortic segments become subject of reduced distension. Since we can safely assume that the main reflection site was not altered, as slipping rigid prints around the aorta segments without causing their compression should not introduce new reflection sites, we can say that the transit time and PWV were not modified by the stiffening. This suggests that measuring the PWV alone might not provide evidence of the presence of a local stiffness 4Conclusion
Our results suggest that the nearer the stiffness is to the ventricle, the more prominent its effect, increasing progressively the left ventricle load. The presence of an atherosclerosis plaque not only limits local aortic buffering and conduit functions, but its effects extend to adjacent sites. Global arterial stiffness index like the PWV might fail to detect regional alterations in wall distension.Acknowledgements
No acknowledgement found.References
1. Mitchell, Gary F., Helen Parise, Emelia J. Benjamin, Martin G. Larson, Michelle J. Keyes, Joseph A. Vita, Ramachandran S. Vasan, and Daniel Levy. Changes in arterial stiffness and wave reflection with advancing age in healthy men and women the Framingham Heart Study. Hypertension 43, no. 6 (2004): 1239-1245
2. Alain Herment, Nadjia Kachenoura, Muriel Lefort, Mourad Bensalah, Anas Dogui, Frédérique Frouin, Elie Mousseaux, and Alain De Cesare. Automated segmentation of the aorta from phase contrast MR images: validation against expert tracing in healthy volunteers and in patients with a dilated aorta. J. Magn. Reson. Imaging, 31(4):881–888, 2010.
3. Cristina Giannattasio, Monica Failla, Guglielmo Emanuelli, Alessandr Grappiolo, Lucia Boffi, Davide Corsi, and Giuseppe Mancia. Local effects of atherosclerotic plaque on arterial distensibility. Hypertension, 38(5):1177–1180, 2001
4. Danial
Shahmirzadi and Elisa Konofagou. Detection of aortic wall inclusions using
regional pulse wave propagation and velocity in silico. Artery research, 6(3):114–123, 2012.
Figures