3210
Factors related to the failure of MR elastography of the liver: multivariate analysis1Radiology, Fukuoka University, Fukuoka, Japan
Synopsis
Seventy consecutive patients with chronic liver diseases and whose R2* values of the liver exceeded 100 s-1 were retrospectively recruited, and factors related to MR elastography failure were analyzed. Iron accumulation which corresponds to R2* value over 200 s-1 and Child-Pugh score 10 are found to be the two independently significant factors that are related to the failure of MR elastography of the liver. For the assessment of the degree of liver fibrosis in those associated with these factors, other modality, such as ultrasonic elastography, may be considered.
INTRODUCTION
MR elastography (MRE) is a recently emerging technique to assess the degree of liver fibrosis in patients with chronic liver diseases 1-3. Its technical success rate is high, although not perfect. Iron accumulation is one of the well-known causes of MRE failure 1,2, due to signal loss of the original gradient-echo or echo-planar images (EPI), however, how much iron accumulation actually bothers MRE has not been clarified. The purpose of this study is to elucidate the factors that are related to MRE failure, particularly the degree of R2* elevation due to iron accumulation.
METHODS
Between November 2012 and July 2016, more than 2000 patients underwent commercially available EPI-based MRE (TR/TE=1000/59 ms, 60 Hz external vibrator, 80 Hz MEG, 4 slices under 16s breath-holding) and IDEAL-IQ (TR/TE/FA=6.6/2.9 ms/3, echo space 0.9, 3 echoes x 2) sequence of the liver at a 3.0T clinical unit in our institute, among whom 70 patients were retrospectively recruited whose R2* values exceeded 100 s-1. There were 61 men and 9 women, and the etiologies of the liver diseases were HCV infection/ HBV infection/ alcoholic liver disease/ nonB-nonC cirrhosis =19/ 24/ 10/ 9/ 8. The liver stiffness of these patients ranged from 1.7 to 11.9 kPa (mean 4.1), and R2* values ranged from 100 to 445 s-1 (mean 154). MRE failure was found in 40 slices (14%) in 20 patients (29%). Factors including age, body mass index, degree of steatosis (fat fraction), liver stiffness, R2* values, and Child-Pugh score, were correlated to the number of slices with MRE failure.RESULTS
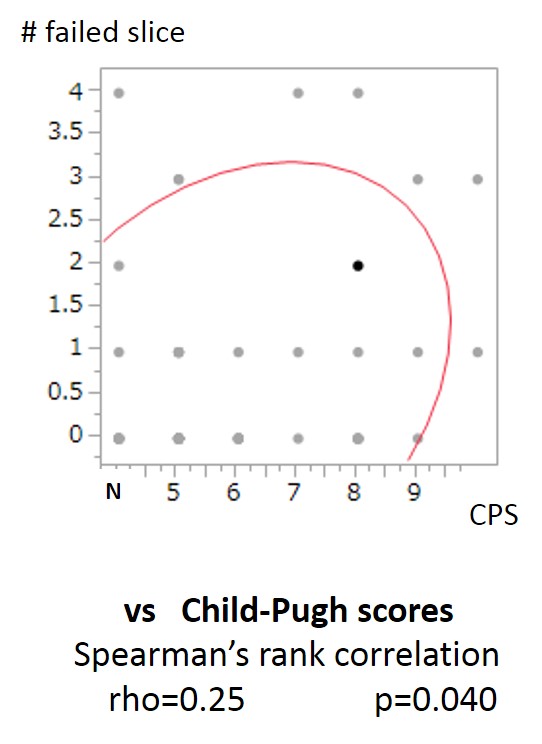
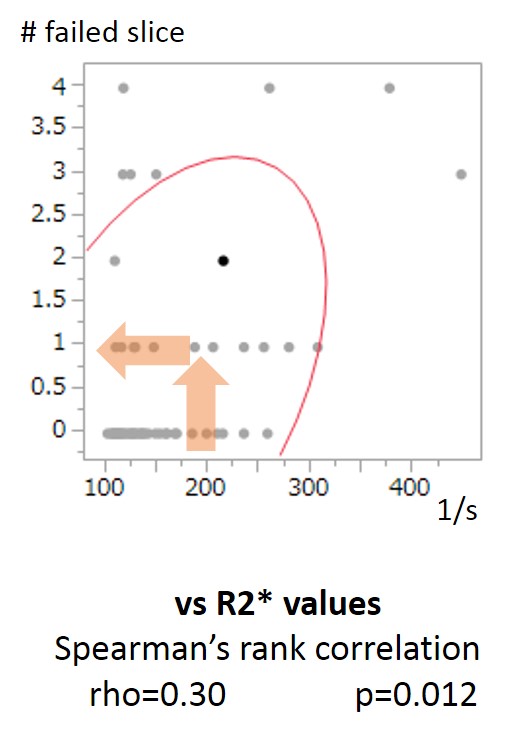
By univariate analysis, age, R2* values, and CPS were found to be significant factors (p<0.05), whereas multivariate (stepwise regression) analysis suggested only R2* values and CPS (10 vs 9 or lower) were the independently significant factors that are related to MRE failure (p<0.05). Spearman’s rank correlation suggested around 200 s-1 or higher R2* value may roughly result in at least one slice MRE failure.CONCLUSION
Iron accumulation which results in R2* elevation over 200 s-1 and CPS 10 may cause at least one slice of MRE failure. For the assessment of the degree of liver fibrosis in those associated with these factors, other modality, such as ultrasonic elatography, may be considered.Acknowledgements
NAReferences
1. Glaser KJ, Manduca A, Ehman RL. Review of MR elastography application and recent developments. JMRI 2012, 36:757-774
2. Venkatesh SK, Yin M, Ehman RL. Magnetic resonance elatography of liver: technique, analysis, and clinical application. JMRI 2013, 37:544-555.
3. Yoshimitsu K, Mitsufuji T, Shingawa Y, et al. MR elastography of the liver at 3.0T in diagnosing liver fibrosis grades: preliminary clinical experience. Eur Radiol 2016, 26:656-663
Figures