3203
Use of intravoxel incoherent motion (IVIM) derived texture parameters in prediction of microvascular invasion of hepatocellular carcinoma (HCC) in patients with hepatitis B virus infection1Department of Radiology, the Third Affiliated Hospital, Sun Yat-sen University (SYSU), Guangzhou, People's Republic of China, 2GE Healthcare MR Research China, Guangzhou, People's Republic of China, 3MR Research China,GE Healthcare, Beijing, 4Mayo Clinic
Synopsis
Hepatocellular carcinoma (HCC) is the most common primary malignancy of the liver worldwide. Microvascular invasion (MVI) is a significant predictor of prognosis and preoperative prediction of MVI is useful for deciding treatment strategy. We assessed the value of ADC and IVIM texture parameters in predicting the MVI of HBV-related HCCs by whole tumor analysis. Our results showed that ADC and IVIM derived texture parameters were useful for the prediction of MVI of HCCs. Texture analysis of ADC and IVIM is a promising method for predicting MVI of HBV-related HCC.
Introduction
Hepatocellular carcinoma (HCC) is the most common primary malignancy of the liver with high malignant degree and mortality rate1.The prognosis of HCC remains unsatisfactory due to the high rate of recurrence. Tumor heterogeneity is an important characteristic of HCC2. Microvascular invasion (MVI) is a strong predictor of recurrence after liver transplantation or hepatic resection3,4. Preoperative diagnosis of MVI could be helpful for the selection of treatment. Some tumor imaging features such as non-smooth tumor margins, peritumorial enhancement5, CT perfusion analysis6, gadoxetic acid enhanced MR7 and apparent diffusion coefficient (ADC) values8 have been shown to be the promising ways to predict MVI in HCC. However, tumor heterogeneity could not be totally reflected by mean values obtained only from a region of interest (ROI) of one slice 9.Intravoxel incoherent motion (IVIM) is a functional MR imaging technique which could reflect the molecular diffusion of water and the microcirculation of the tumor10,11.Texture analysis is a method which could capture the intratumoral heterogeneity9,12. This study aimed to investigate the performance of IVIM texture parameters in detecting MVI in HBV-related HCCs.Methods
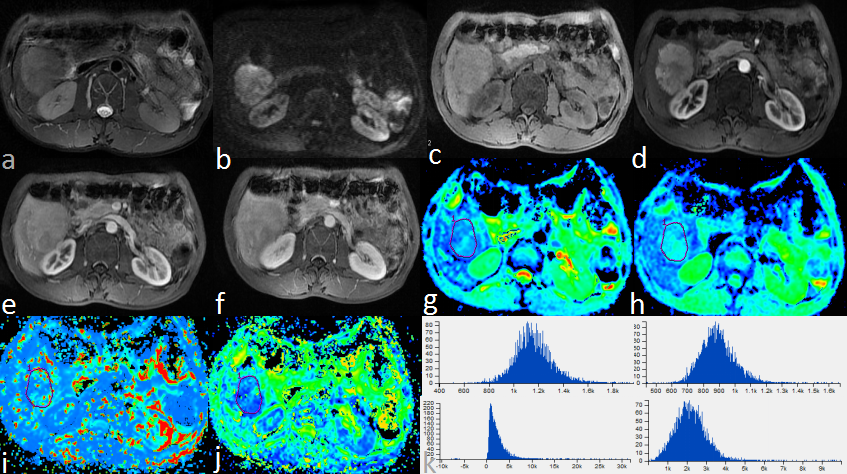
The study was approved by the institutional review board and written informed consents were obtained from each recruited patient.97 patients (85 males and 12 females; age range, 35-77 years; mean, 60.2 years) were included in our study according to the following criteria: (a) patients with chronic HBV infection and pathologically confirmed HCC after surgical resection or liver transplantation,(b) preoperative MR examination was performed within one month before surgery, (c) without any preoperative anticancer treatment such as transarterial chemoembolization (TACE) and radiofrequency ablation (RFA), (d) without distinct motion artifacts or slice misregistration, (e) the lesions were more than 1 cm in diameter, (f) without macrovascular invasion on any imaging modalities. The patients were classified into two groups according to pathological results: HCC with MVI (n=49) and without MVI (n=48). All subjects underwent MRI exam using a 3.0T whole-body MRI scanner (Discovery MR750, GE Healthcare, Milwaukee, WI). Respiratory-triggered diffusion-weighted imaging (DWI) were performed using 11 b values (b=0, 30, 50, 100, 150, 200, 300, 500, 800, 1000, 1500 sec/mm2).Regions of interests (ROIs) were placed on the ADC maps with reference to the T2WI images by manually tracing the margin of each slice of the lesion. All ROIs were merged into a volume of interest (VOI) which covers the whole tumor and was copied to D, D* and f maps generated from the IVIM automatically. Texture parameters of ADC, D, D* and f of the whole tumor were calculated based on histogram and grey level co-occurrence matrix (GLCM) algorithm9 (Omni-Kinetics, GE Healthcare). The values of MVI (+) and MVI (-) group were compared with Student t test or Mann–Whitney U test depending on the statistical distribution of the data.Results
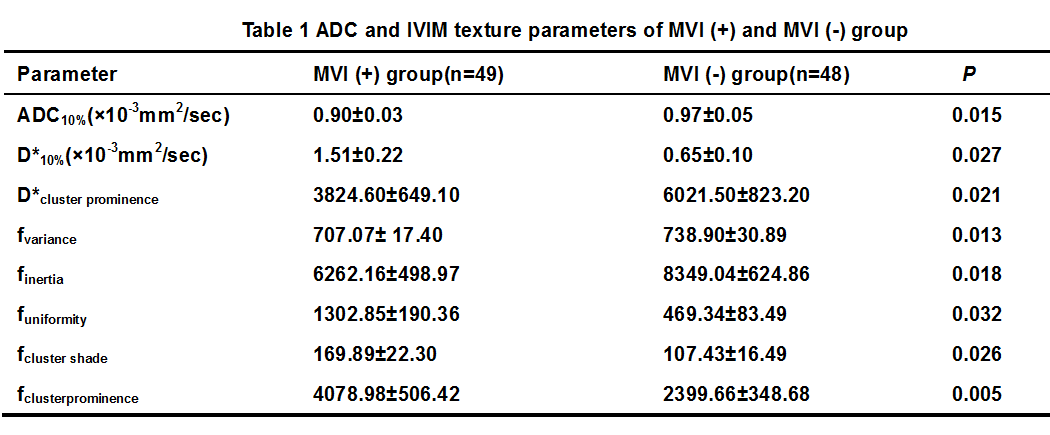
10th percentile of ADC value, cluster prominence of D* values, variance and inertia of f values of the MVI (+) group were significantly lower than those of MVI (-) group (P=0.015,0.02,0.013 and 0.018, respectively). 10th percentile of D*, uniformity, cluster shade and cluster prominence of f values of the MVI (+) group were significantly higher than those of the MVI (-) group (P=0.027, 0.032, 0.026 and 0.005, respectively). On the other hand, the mean values of ADC and IVIM metrics were not significantly different between the MVI (+) and MVI (-) group.Discussion
In our study, tumor heterogeneity was quantified by texture analysis of the whole tumor. Using whole tumor analysis, the heterogeneity of the HCC may be captured better compared with single slice analysis9. The diffusion and perfusion of the tumor was reflected by ADC and IVIM metrics. Our study showed that the ADC and IVIM derived texture parameters have the potentials of predicting MVI in HBV-related HCCs. Further studies are needed to investigate the value of texture parameters of ADC and IVIM as biomarkers in predicting the MVI of HBV-related HCC.Conclusion
In summary, texture parameters of ADC and IVIM could be useful for predicting the MVI of HBV-related HCCs preoperatively and they may play an important role in the treatment strategy selection of HBV-related HCCsAcknowledgements
NoReferences
1.de Martel C, Maucort-Boulch D, Plummer M, et al. World-wide relative contribution of hepatitis B and C viruses in hepatocellular carcinoma[J]. Hepatology,2015,62(4):1190-1200.
2.Lu L, Hsu C, Hsu C, et al. Tumor Heterogeneity in Hepatocellular Carcinoma: Facing the Challenges[J]. Liver Cancer,2016,5:128-138.
3.Colecchia A, Schiumerini R, Cucchetti A, et al. Prognostic factors for hepatocellular carcinoma recurrence[J]. World J Gastroenterol, 2014,20:5935-5950.
4. Sumie S, Kuromatsu R, Okuda K, et al. Microvascular Invasion in Patients with Hepatocellular Carcinoma and Its Predictable Clinicopathological Factors[J]. Ann Surg Oncol,2008,15:1375-1382. 5.Renzulli M, Brocchi S, Cucchetti A, et al. Can Current Preoperative Imaging Be Used to Detect Microvascular Invasion of Hepatocellular Carcinoma?[J]. Radiology,2016,279:432-442.
6. Wu D, Tan M, Zhou M, et al. Liver computed tomographic perfusion in the assessment of microvascular invasion in patients with small hepatocellular carcinoma[J]. Invest Radiol,2015,50:188-194.
7.Kim K A, Kim M, Jeon H M, et al. Prediction of microvascular invasion of hepatocellular carcinoma: Usefulness of peritumoralhypointensity seen on gadoxetate disodium-enhanced hepatobiliary phase images[J]. J MagnReson Imaging,2012,35:629-634.
8.Xu P, Zeng M, Liu K, et al. Microvascular invasion in small hepatocellular carcinoma: Is it predictable with preoperative diffusion-weighted imaging?[J]. J Gastroenterol Hepatol,2014,29:330-336.
9. Nougaret S, Vargas H A, Lakhman Y, et al. Intravoxel Incoherent Motion-derived Histogram Metrics for Assessment of Response after Combined Chemotherapy and Radiation Therapy in Rectal Cancer: Initial Experience and Comparison between Single-Section and Volumetric Analyses[J]. Radiology,2016,280:446-454.
10.LeBihan D, Breton E, Lallemand D, et al. Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging[J]. Radiology,1988,168:497-505.
11.Woo S, Lee J M, Yoon J H, et al. Intravoxel incoherent motion diffusion-weighted MR imaging of hepatocellular carcinoma: correlation with enhancement degree and histologic grade[J]. Radiology,2014,270:758-767.
12. Huang Y, Liang H, Yang Z, et al. Value of MR histogram analyses for prediction of microvascular invasion of hepatocellular carcinoma[J]. Medicine,2016,95:e4034.
Figures