3200
Quantitative Assessment of Liver Fibrosis using MR-Phase Information1Department of Radiology, Fukuoka University Chikushi Hospital, Fukuoka, Japan, 2Department of Medical Physics in Advanced Biomedical Sciences, Faculty of Life Sciences, Kumamoto University, Kumamoto, Japan, 3Department of Radiology, Fukuoka University Hospital, Fukuoka, Japan
Synopsis
The aim of this study was to evaluate a potential of MR-phase information for a quantification of liver fibrosis. We measured phase value of the liver and examined the correlation between that value and the stage of fibrosis. Additionally, we also evaluate the correlations among phase value and the serum biomarkers of fibrosis and cirrhosis. The phase value showed high statistical correlation to stages of fibrosis, and to be linearly proportional to the following biomarkers; PLT, APRI, FIB-4 index. In conclusion, MR-phase information may is to be a noninvasive quantitative tool for liver fibrosis and its progression.
PURPOSE
Liver fibrosis leading to cirrhosis is a common pathology arising from various causes 1, and accurate assessment of liver fibrosis is important for prognosis, since the risk of hepatocarcinogenesis becomes higher as liver fibrosis progresses. Recently, several MRI methods to assess liver fibrosis were developed and already worked on clinical MRI. It was reported that MR-phase information as a tool of diagnosis for fibrosis was especially sensitive to tissue changing due to fibrosis 2. Therefore, it is expected that the liver fibrosis may be quantified by using phase information because it is quantitative value. The purpose of this study was to show a potential of phase information to quantify and the liver fibrosis by comparison with serum biomarkers, which would be applicable for practical clinical use.METHODS
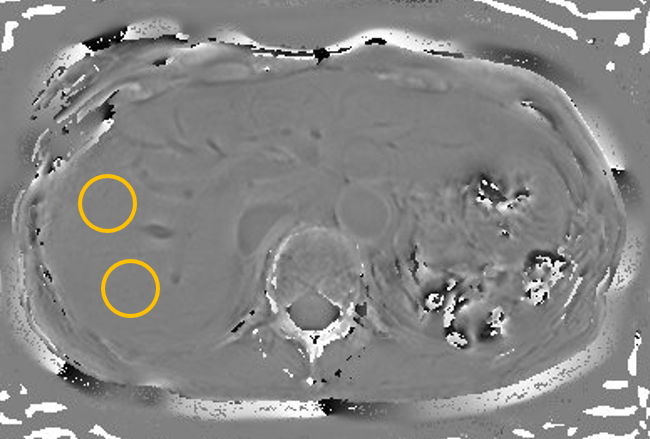
This study was approved by the institutional review board of Fukuoka University Chikushi Hospital. Subjects of this study were 50 patients with liver MRI examinations (28 males and 22 females, mean age 66.75 ± 12.29 years, age range 35-82 years). All studies were performed on a 3.0T-MR system (Ingenia, Philips Healthcare, The Netherlands). T2*-weighted 2D GRE images were acquired with phase images. Scan parameters were as follows: repetition time 150 msec, echo time 10 msec, field of view 350 × 300 mm, scan matrix 300 x 300, slice thickness 8 mm, slice gap 1 mm, flip angle 20 degrees, slices 22, pixel band width 218 Hz. Each scan had been done by two breath holdings (total scan duration was 40 ms including break time). We used phase difference enhanced imaging (PADRE) to obtain unwrapped phase image and measured averaged phase value in region of interest located on the right hepatic lobe, including segment 5 to 8 (Fig. 1). Liver fibrosis was staged by the aspartate aminotransferase (AST)-to-platelet (PLT) ratio index (APRI) with the following cutoffs for stratify patients; APRI ≤ 0.5 (no significant fibrosis), 0.5 < APRI ≤ 1.5 (mild to moderate fibrosis) and APRI > 1.5 (cirrhosis) 3. The correlation between phase value and fibrosis and/or cirrhosis were statistically examined using PLT, AST/ the alanine aminotransferase ratio (AAR), APRI and FIB-4 index 4-6.RESULTS
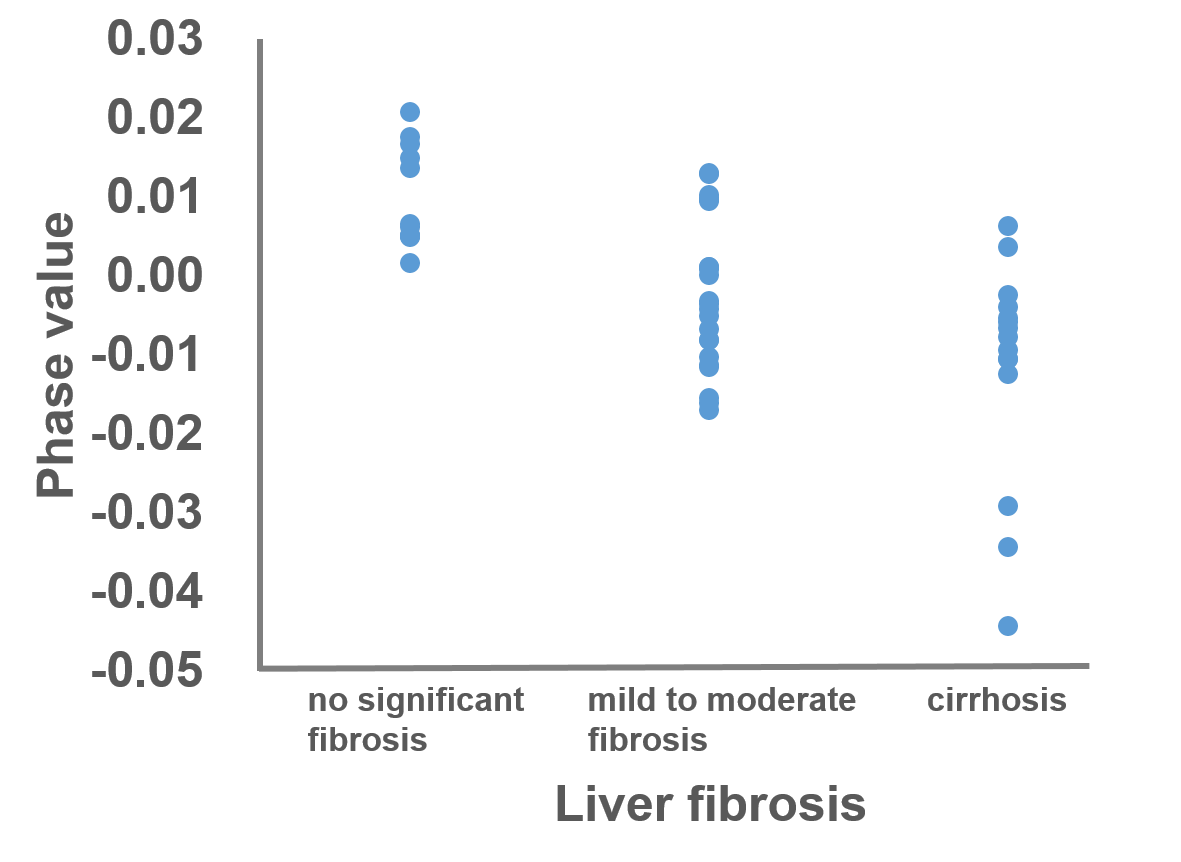
The phase values were statistically significantly different among different fibrosis stages, which were decreased as stage progressed (ρ = -0.61, P < 0.001) (Fig. 2). The phase value also showed significant positive correlations with PLT (r = 0.70, P < 0.001), significant negative correlations with APRI (r = -0.69, P < 0.001) and FIB-4 index (r = -0.75, P < 0.001). There was no significant correlation between the phase value and AAR (r = -0.02, P = 0.81) (Fig. 3).DISCUSSION
The phase value showed negative value and negative proportionality to TE, which was to be collagen fiber accumulated with iron or paramagnetic materials depositions. Additionally, the phase value of liver showed significant correlations with PLT, APRI, and FIB-4 index, but no correlation with AAR. Previous study has reported that AAR was not useful in predicting the degree of fibrosis 7 because AAR is the value reflecting the inflammatory than fibrosis. In summary, results in this study showed that the phase value potentially assesses the stage of liver fibrosis and we may quantify the progression of liver fibrosis by phase information.CONCLUSION
The phase information is to be a noninvasive quantitative tool for liver fibrosis and its progression. In future, by appropriate phase selection, we may realize qualitative phase-enhanced images such as SWI and PADRE for liver fibrosis.Acknowledgements
No acknowledgement found.References
1. Rockey DC. Hepatic fibrosis, stellate cells, and portal hypertension. Clin Liver Dis. 2006;10(3):459-479
2. Balassy C, Feier D, Peck-Radosavljevic M, et al. Susceptibility-weighted MR imaging in the grading of liver fibrosis: a feasibility study. Radiology. 2014;270(1):149-158
3. Snyder N, Nguyen A, Gajula L, et al. The APRI may be enhanced by the use of the FIBROSpect ? in the estimation of fibrosis in chronic hepatitis C. Clin Chim Acta. 2007;381(2):119-123
4. Poynard T, Bedossa P. Age and platelet count: a simple index for predicting the presence of histological lesions in patients with antibodies to hepatitis C virus. METAVIR and CLINIVIR Cooperative Study Croups. J Viral Hepat. 1997;4(3):199-208
5. Giannini E, Risso D, Testa R. Transportability and reproducibility of the AST/ALT ratio in chronic hepatitis C patients. Am J Gastroenterol. 2001;96(3):918-919
6. Vallet-Pichard A, Mallet V, Nalpas B, et al. FIB-4: an inexpensive and accurate marker of fibrosis in HCV infection. Comparison with liver biopsy and fibrotest. Hepatology. 2007;46(1):32-36
7. Eminler AT, Ayyildiz T, Irak K, et al. AST/ALT ratio is not useful in predicting the degree of fibrosis in chronic viral hepatitis patients. Eur J Gastroenterol Hepatol. 2015;27(12):1361-1366
Figures