3178
Clinical Robustness of Accelerated and Optimized Abdominal Diffusion Weighted Imaging1Department of of Diagnostic and Interventional Radiology, University Hospital of Tuebingen, Tuebingen, Germany, 2Section on Experimental Radiology, Department of Diagnostic and Interventional Radiology, University Hospital of Tuebingen, Tuebingen, Germany, 3Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
We evaluated the robustness of an accelerated and optimized diffusion-weighted sequence using the simultaneous-multislice (SMS) technique for scan time reduction and a 3D Diagonal diffusion mode to optimize image quality in clinical routine. 152 patients received clinically indicated abdominal MRI including the optimized diffusion-weighted sequence (DWIOPT). A subgroup of 41 patients additionally received a standard diffusion-weighted sequence (DWISTD) as reference. Qualitative and quantitative image parameters were evaluated. In the interindividual comparison, DWIOPT proved equal to superior to DWISTD with comparable ADC-values. In the patients receiving DWIOPT only, image quality maintained substantial proving constant and stable results in a large cohort.
Purpose
While diffusion-weighted imaging (DWI) is an established technique in MR-imaging and has proven helpful in the evaluation of therapeutic response in oncological treatment, 1,2 scan time reduction has been playing a major role in a widespread application in clinical routine. To counteract this shortcoming, the SMS technique excites several slices simultaneously and uses parallel imaging to calculate individual images from the collapsed multislice images. In DWI, usually a trace-weighted approach is employed where an isotropic diffusion-weighted trace image is calculated from images acquired with different gradient directions. However, blurring in the trace-weighted image may occur due to different eddy-current-induced distortions of the individual diffusion-weighted images. In case of isotropic diffusion, which is expected for malignancies, 3 the trace-weighted diffusion mode can be replaced by a 3D Diagonal mode using a single gradient direction to avoid the blurring.
Thus, purpose of this study was to assess the robustness of an accelerated and optimized prototype diffusion-weighted sequence in clinical routine abdominal imaging using the simultaneous-multislice (SMS) technique for scan time reduction and a 3D Diagonal diffusion mode to optimize image quality.
Methods
A total of 152 patients (88 male, 64 female; mean age 62 years) were included in this study. All received clinically indicated abdominal MRI including an optimized prototype diffusion-weighted sequence (DWIOPT: TR/TE 3100/56 milliseconds; b-values 50, 400 and 800 s/mm²; diffusion mode 3D Diagonal; SMS factor 2; scan time 1:44 minutes) in free-breathing. A subgroup of 41 patients (21 male, 20 female; mean age 62 years) additionally received a standard diffusion-weighted sequence (DWISTD: TR/TE 5100/60 milliseconds; b-values 50, 400 and 800 s/mm²; diffusion mode 4-scan Trace; scan time 2:35 minutes) in free-breathing as reference. Image quality criteria and lesion conspicuity in DWISTD and DWIOPT were rated on a 5-point Likert scale (5 = excellent). ADC values were measured in a region-of-interest-based manner. Qualitative and quantitative image parameters of DWISTD and DWIOPT were compared interindividually within the subgroup (using Dunn-Bonferroni post hoc test for pairwise comparisons in case of significant p-values in the Wilcoxon-signed-rank test/student´s t-test). P-values < 0.05 were considered significant.Results
Interindividually DWIOPT proved superior to DWISTD in comparison of overall image quality and contour sharpness of the right and left hepatic lobe (DWIOPT: overall image quality 4.6±0.7, contour sharpness right/left hepatic lobe 4.6±0.5/4.3±0.5; DWISTD: overall image quality 4.2±0.8, contour sharpness right/left hepatic lobe 4.3±0.8/4.0±0.9; p=.025, p=.045 and p=.045); lesion conspicuity was comparable in DWIOPT and DWISTD (4.0±1.7 vs. 4.4±1.3; p=.461), measured ADC values showed no statistically significant difference (ADCOPT vs. ADCSTD: right hepatic lobe p=.107; kidney p=.0980). In the patients receiving DWIOPT only overall image quality (4.7±0.6), contour sharpness of right/left hepatic lobe (4.7±0.5/4.4±0.6, respectively) and lesion conspicuity (4.7±0.6) was rated very high.Discussion
In this study, we could demonstrate the robustness of an accelerated and optimized DWI in a clinical setting. Scan time was reduced by one third, and overall image quality in the interindividual comparisons was rated very high with equivalent to superior quality in the DWIOPT as compared to DWISTD as well as equivalently high lesion conspicuity in both sequences. Image quality ratings and lesion conspicuity in patients without DWISTD as reference were also substantial, proving constant and stable results in a larger cohort, and thus, demonstrating consistency between our results and the results of previous evaluations in smaller cohorts.4,5
We noticed a moderate increase in sharpness of the liver contour in DWIOPT compared to the standard sequence. This increase can be explained by the one diffusion direction of the 3D Diagonal mode. In this mode, the distortions induced by eddy currents in the individual diffusion-weighted EPI images are identical, increasing the sharpness of the averaged diffusion-weighted image used for diagnosis. However, we expressly point out that a 3D Diagonal mode can lead to direction dependent signal alteration if a strong diffusion anisotropy of the tissue (e.g. renal medulla) or lesion under study is expected.
No statistically significant differences in ADC values in liver, kidney or lesions were detected. This is consistent with a previously performed study comparing SMS-accelerated DWI to conventional DWI at 3 T in the liver describing no statistically significant differences in ADC values in normal parenchyma as well as in liver lesions.4
Conclusion
DWI of the abdomen can be accelerated and optimized integrating the SMS technique and a 3D Diagonal diffusion mode. In a large patient cohort, this approach proved stable and of superior image quality while maintaining similar ADC values compared to standard diffusion-weighted imaging. It is, thus, recommendable for application in daily routine.Acknowledgements
The authors would like to thank Mathias Kündel and Ayser Birinci-Aydogan for their encouragement throughout this project.References
1. Bains LJ, Zweifel M, Thoeny HC. Therapy response with diffusion MRI: an update. Cancer Imaging. 2012;12(2):395-402.
2. Kartalis N, Lindholm TL, Aspelin P, Permert J, Albiin N. Diffusion-weighted magnetic resonance imaging of pancreas tumours. European Radiology. 2009;19(8):1981-1990.
3. Padhani AR, Koh D-M, Collins DJ. Whole-Body Diffusion-weighted MR Imaging in Cancer: Current Status and Research Directions. Radiology. 2011;261(3):700-718.
4. Obele CC, Glielmi C, Ream J, et al. Simultaneous Multislice Accelerated Free-Breathing Diffusion-Weighted Imaging of the Liver at 3T. Abdominal Imaging. 2015;40(7):2323-2330.
5. Taron J, Martirosian P, Schwenzer NF, et al. Scan time minimization in hepatic diffusion-weighted imaging: evaluation of the simultaneous multislice acceleration technique with different acceleration factors and gradient preparation schemes. Magnetic Resonance Materials in Physics, Biology and Medicine. 2016:1-11.
Figures
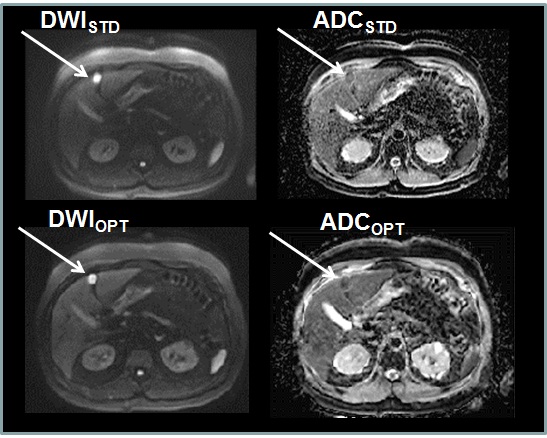
Figure 1 Image quality of DWISTD and DWIOPT in a patient with metastatic colorectal cancer
Images obtained in a 63-year old male patient with metastatic colorectal cancer. Image set consisting of b = 800 s/mm² (DWISTD/DWIOPT) and the corresponding ADC map (ADCSTD/ADCOPT). Very high overall image quality in DWIOPT and high overall image quality in the DWISTD. Superior image sharpness in DWIOPT as compared to the DWISTD. Slice position varies slightly due to different breathing cycles.
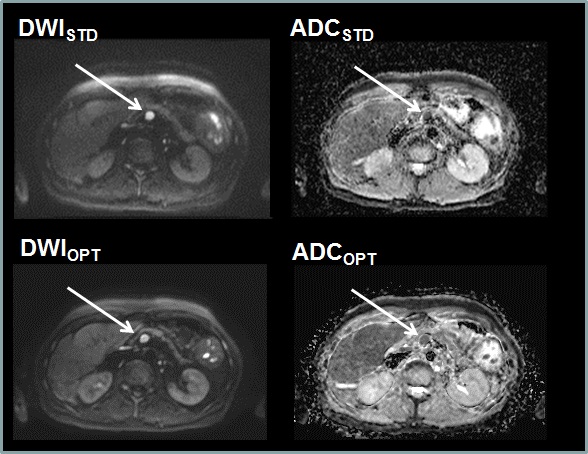
Figure 2 Image quality of DWISTD and DWIOPT in a patient with metastatic ovarian cancer
Images obtained in a 68-year old female patient with metastatic ovarian cancer. Image set consisting of b = 800 s/mm² (DWISTD/DWIOPT) and the corresponding ADC map (ADCSTD/ADCOPT). Very high overall image quality in DWIOPT and high overall image quality in the DWISTD. Superior image sharpness in DWIOPT as compared to the DWISTD. Slice position varies slightly due to different breathing cycles.
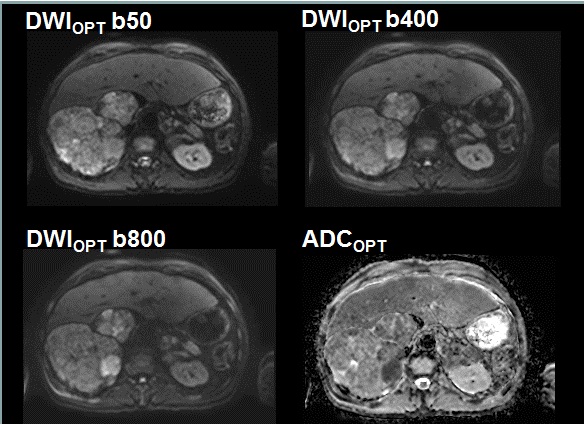
Figure 3 Image quality of DWIOPT in a patient with renal cell carcinoma
Images obtained in a 58-year old male patient with renal cell carcinoma. Image set consisting of b = 50, 400 and 800 s/mm² (DWIOPT b50/b400/b800) and the corresponding ADC map (ADCOPT). Follow-up was performed with standard abdominal MRI protocol including DWIOPT only with very high image quality in b50, b400 and b800 s/mm² as well as the corresponding ADC map.