3164
Contribution of DKI and IVIM to liver T1rho imaging in the prediction of hepatitis B virus-related liver fibrosis1Tianjin First Center Hospital, Tianjin, People's Republic of China, 2Philips healthcare, Beijing, People's Republic of China
Synopsis
This study evaluated the individual T1rho and combined performances of T1rho, IVIM and DKI in predicting HBV related liver fibrosis. Twenty-two patients with HBV related liver fibrosis and twenty healthy control subjects were underwent whole-liver T1rho MR imaging, IVIM and DKI. The T1rho, D, D*, f , MD and MK values were compared between the two groups, and then the single and combined diagnostic efficiency of T1rho, IVIM and DKI was analyzed. Our results showed liver T1rho and MK increased and D, f, MD decreased in normal control group, and liver T1rho and MD had significantly difference between the two groups. T1rho had a moderate diagnostic efficiency, IVIM and DKI had a mild diagnostic efficiency to detect fibrosis. While, the combination of T1rho, IVIM and DKI improved the diagnostic efficiency significantly and had a good diagnostic efficiency to detect fibrosis. We conclude T1rho can be used to predicting liver fibrosis effectively, and IVIM and DKI can effectively complement existing T1rho MR imaging in predicting of liver fibrosis.
Purpose
Due to possible reversibility of hepatic fibrosis and even early cirrhosis, early and accurate diagnosis of liver fibrosis is important to allow an appropriate treatment strategy to be chosen and to predict the prognosis of patients[1]. On pathomorphological analysis, liver fibrosis is characterized by excess accumulation of macromolecules in the extracellular matrix (ECM), inflammation reflection and sinusiod capillarization, liver fibrosis is associated with progressive restriction of diffusion motion and perfusion changes[2,3]. Prior studies have demonstrated the possible diagnostic efficiency of T1rho, IVIM in predicting fibrosis[4,5]. Based on the imaging theory, DKI may also be used to evaluate the tissue complexity of liver fibrosis[6]. So the purpose of this study was to evaluate the individual T1rho and combined performances of T1rho, IVIM and DKI in predicting HBV related liver fibrosis.Materials and methods
This single-center prospective study was approved by the institutional review board, and the requirement for informed consent was waived. Twenty-two patients with HBV infection and a pathological diagnosis of liver fibrosis (F/M=8/14, mean age=37.2±8.70 years, range 27-58 years) and twenty patients without chronic liver disease (healthy liver group, F/M=7/13, mean age=41.4±4.91 years, range 27-46 years) were underwent whole-liver T1rho MR imaging, IVIM and DKI. The T1rho, IVIM (true diffusion coefficient (D), pseudodiffusion (D*), perfusion fraction (f)) and DKI parameters (mean diffusion (MD), mean kurtosis (MK) values) were measured and compared between the fibrosis liver group and healthy liver group. The discriminative abilities of the different parameters were compared by means of receiver operating characteristic (ROC) curve and area under the ROC curve (AUC) analysis.Results
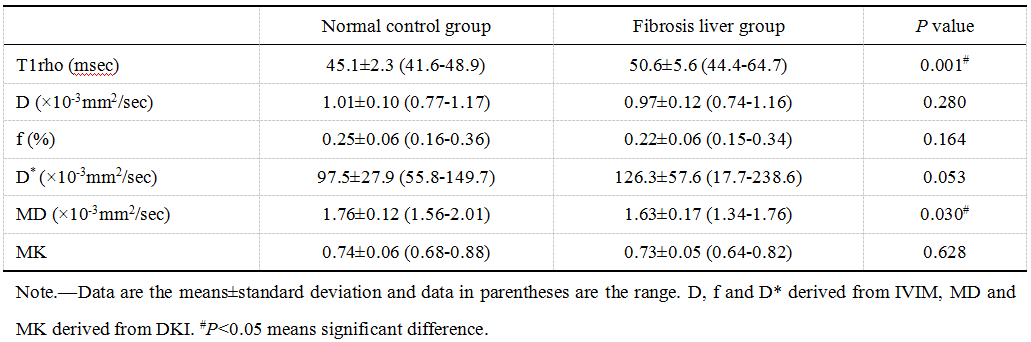
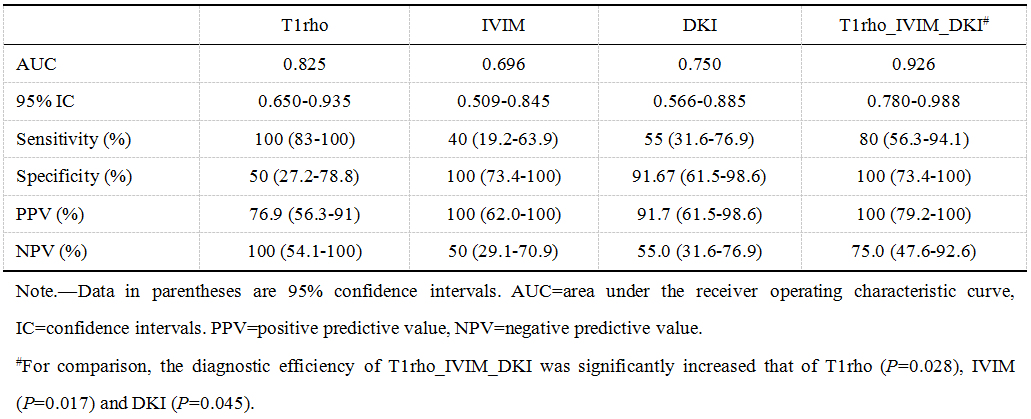
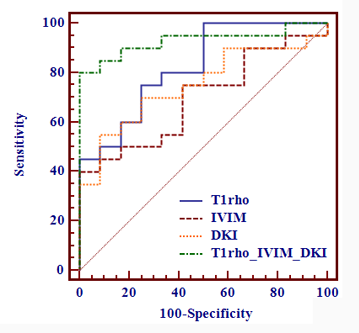
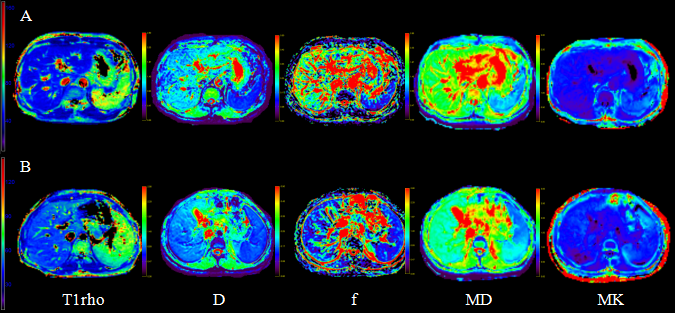
MR parameters derived from T1rho, IVIM and DKI were compared between the two groups and summarized in table 1. Individual and combined diagnostic efficiency of T1rho, IVIM and DKI were summarized in table 2 and Fig.1. Typical parametric images of the two groups are demonstrated in Fig.2. Both in normal control group and fibrosis group, D* values were variable when measured, so it was not compared between the two groups. Compared with fibrosis liver group, liver T1rho and MK increased and D, f, MD decreased in normal control group. Liver T1rho and MD (P<0.05) but not D, f and MK (P>0.05), were significantly different between the normal and fibrosis groups. The AUC values were observed for T1rho (0.825), IVIM (0.696) and DKI (0.750). The combination of T1rho, IVIM and DKI had an AUC significantly increased to 0.926 and provided 80% sensitivity and 100% specificity for diagnosis of liver fibrosis.Discussion
In this study, T1rho, MK increased and D, f, MD decreased in fibrosis liver group compared to control group, which might indicate the increased macromolecules in the ECM, restriction of diffusion motion, tissue complexity and decreased perfusion. D* values were variable in this study, same to the previous study[7]. This might indicate that only f values could be used to evaluate perfusion changes when IVIM was used. T1rho had a moderate diagnostic efficiency, and the combination of T1rho, IVIM and DKI had a good diagnostic efficiency in predicting liver fibrosis. Therefore, the combination of T1rho, IVIM and DKI can provide more accurate and overall assessment of the pathomorphological changes in liver fibrosis.Conclusion
T1rho can be used to predicting liver fibrosis effectively, and IVIM and DKI can effectively complement existing T1rho MR imaging in predicting of liver fibrosis.Acknowledgements
No.References
1. Marcellin P, Gane E, Buti M, et al. Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year-label follow-up study. Lancet. 2013;381(9865):468-475.
2. Novo E, Cannito S, Paternostro C, Bocca C, Miglietta A, Parola M. Cellular and molecular mechanisms in liver fibrogenesis. Arch Biochem Biophys. 2014;548:20-37.
3. Pandharipande PV, Krinsky GA, Rusinek H, Lee VS. Perfusion imaging of the liver: current challenges and future goals. Radiology. 2005;234(3):661-673.
4. Allkemper T, Sagmeister F, Cicinnati V, et al. Evaluation of fibrotic liver disease with whole-liver T1ρ MR imaging: a feasibility study at 1.5 T. Radiology. 2014;271(2):408-415.
5. Lu PX, Huang H, Yuan J, et al. Decreases in molecular diffusion, perfusion fraction and perfusion-related diffusion in fibrotic livers: aprospective clinical intravoxel incoherent motion MR imaging study. PLoS One. 2014;9(12):e113846.
6. Goshima S, Kanematsu M, Noda Y, Kondo H, Watanabe H, Bae KT. Diffusion kurtosis imaging to assess response to treatment in hypervascular hepatocellular carcinoma. AJR Am J Roentgenol. 2015;204(5):W543-549.
7. Kakite S, Dyvorne H, Besa C, et al. Hepatocellular carcinoma: short-term reproducibility of apparent diffusion coefficient and intravoxel incoherent motion parameters at 3.0T. J Magn Reson Imaging. 2015;41(1):149-156.
Figures