3163
Identification and Measurement of Anatomical Landmarks Using Fetal Cardiac Cine MRI in Comparison with the Clinical Gold Standard Echocardiography1Department of Radiology, University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 2Center for Biomedical Imaging (CIBM), Lausanne, Switzerland, 3Department of Pediatrics, University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 4Department of Gynecology-Obstetrics, University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland
Synopsis
The recent development of a self-gated framework to reconstruct cardiac cine MR images without the need for an external ECG signal has opened the door to prenatal cardiac examination with MRI. This study investigates the potential of this technique for fetal cardiac MRI and compares its performance with the clinical gold standard echocardiography. Standard views from clinical fetal echocardiographic examinations were acquired with both imaging modalities and two experienced readers independently compared them qualitatively and quantitatively. The results showed good agreement between the two modalities and validate the use of MRI for prenatal evaluation of the heart.
Purpose
Congenital heart defects (CHDs) affect about 1% of births in the United States1 and are responsible for 30% to 50% of mortality caused by birth defects.2 Currently, fetal echocardiography is the only imaging modality used in clinical settings to assess the fetal cardiovascular system. However, despite common prenatal ultrasound screening, the rate of prenatal detection of CHDs requiring surgical intervention is only 42%3 and it was shown that missed or delayed diagnoses of CHD may lead to mortality.4 It is therefore paramount for patients with critical CHDs to have an alternative imaging modality available when ultrasonographic examination reaches its limits: early or late gestational age, suboptimal fetal position, maternal habitus, multiple gestations, oligohydramnios and poor ultrasonographic windows. Cardiac MRI offers a non-invasive and safe alternative to echocardiography, but has proven to be particularly challenging for fetal cardiac imaging because of the absence of a fetal ECG signal to synchronize MRI data acquisition. A recently developed self-gated framework,5,6 which combines a continuous golden-angle radial data acquisition with a k-t sparse SENSE approach to reconstruct cardiac cine MR images without the need for an external ECG signal, offers a solution to this problem. This study investigates the potential of this technique for fetal cardiac cine MRI and compares its performance with the clinical gold standard echocardiography.Methods
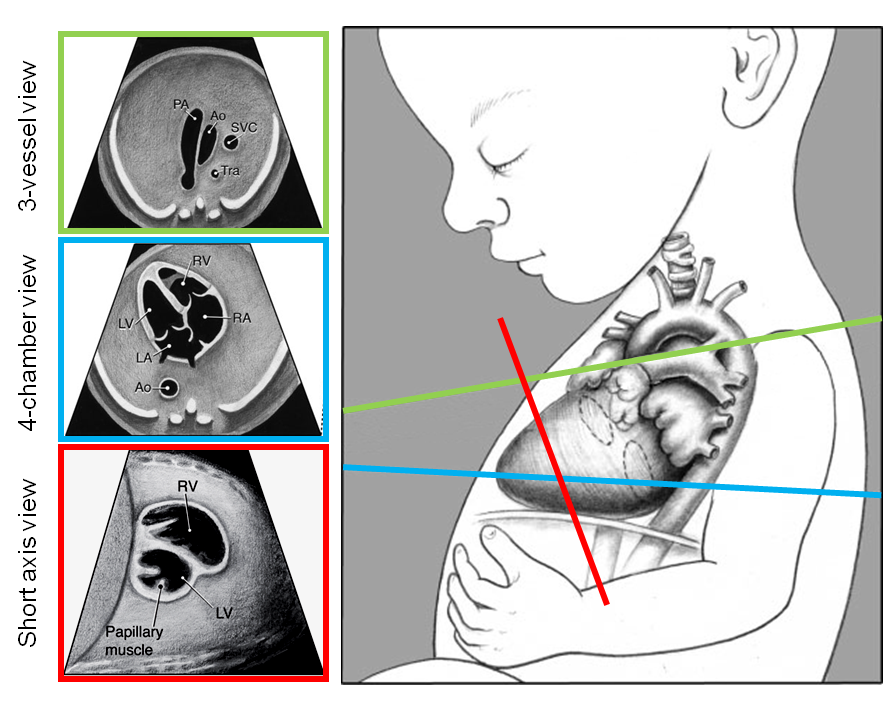
MR Data Acquisition: MR imaging was performed on 6 pregnant patients (gestational age 30±2 weeks) within a week of their echocardiographic examination. Data were acquired on a 1.5T clinical scanner (MAGNETOM Aera, Siemens Healthcare) using a free running 2D golden-angle radial trajectory bSSFP sequence with an 18-channel body coil and a 32-channel spine coil. Sequence parameters included TE/TR=1.99/4.1ms, FOV=260x260mm2, matrix size=256x256pixel, voxel size=1.0x1.0x4.0mm3, RF excitation angle=70°, bandwidth=1028Hz/pixel, acquisition time=6.7s per slice during a breath hold. Three specific views (four-chamber, three-vessel and short-axis, Fig 1) used in standard clinical fetal echocardiographic examinations7 were acquired to assess the fetal cardiac anatomy.
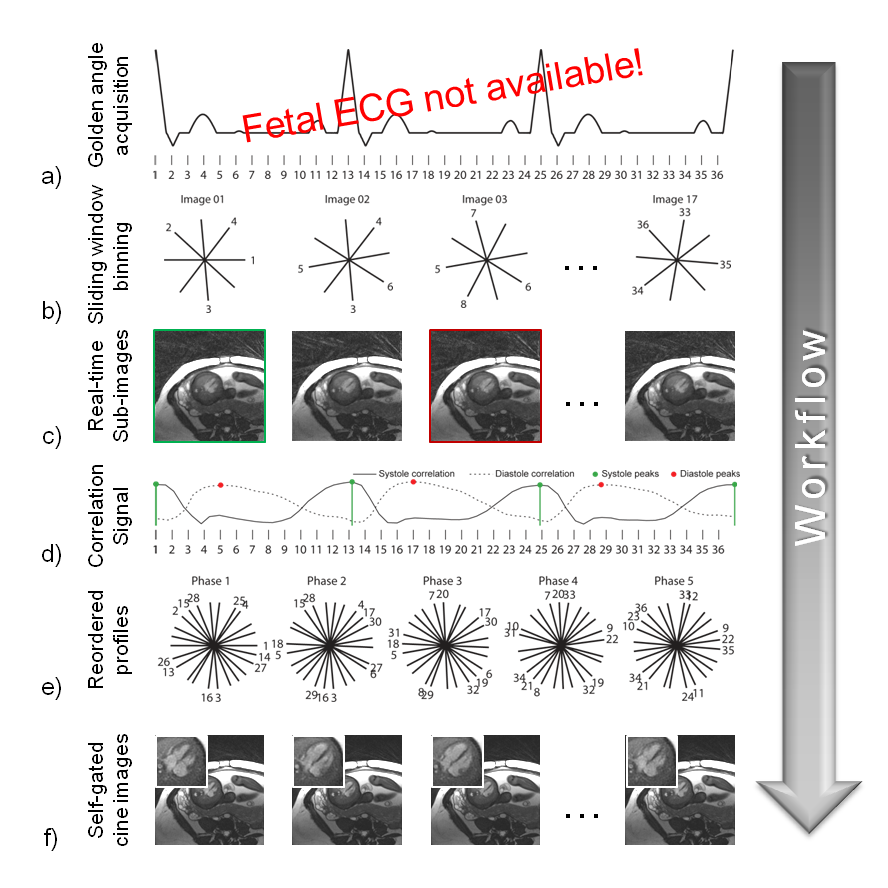
MR Cine Reconstruction: MR cine images with a temporal resolution of 12.5ms (bin width of 25ms, 50% view sharing) were reconstructed using the self-gated framework previously reported.5,6 A brief overview of the reconstruction pipeline is provided in Fig 2.
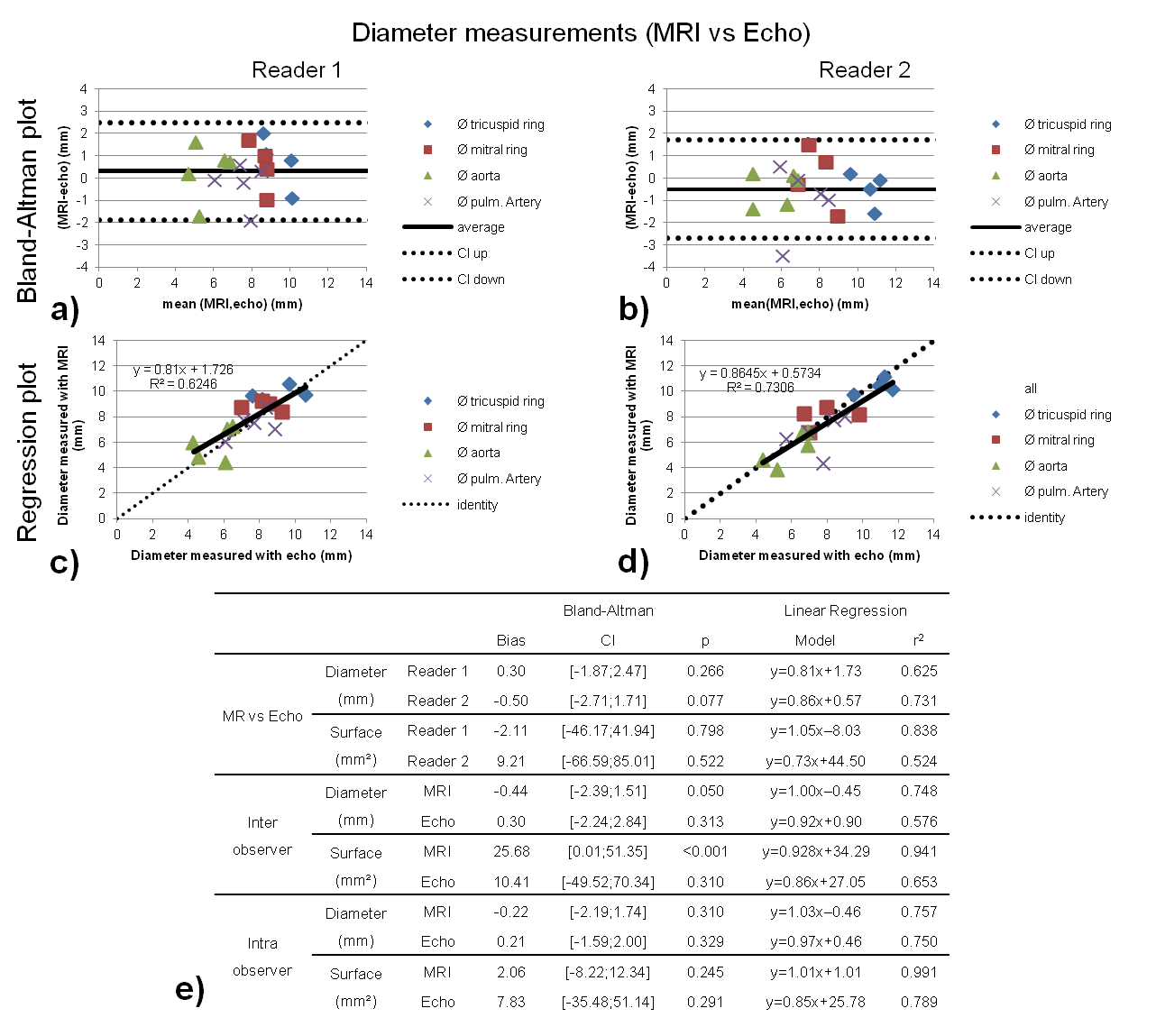
Image Assessment: Echocardiographic and MR cine images of the three specific views were assessed both qualitatively and quantitatively. For the qualitative assessment, two readers independently scored the visibility and delineation of 13 anatomical structures of the fetus’ heart (Fig 1) on a 2-point scale (1: visible, 0: not visible). Quantitative comparison of the imaging modalities included measurement of the diameters of the 1) tricuspid valve ring, 2) mitral valve ring, 3) aorta, 4) main pulmonary artery, and 5) the surface of the left ventricle in systole and diastole on the short axis view. Bland–Altman plots, linear regressions, and paired two-tailed Student’s t-test with p<0.05 considered statistically significant were used to compare the two imaging modalities. Inter- and intra-observer variability analyses were performed for both MR and echography.
Results
Self-gated MR cine images were successfully reconstructed for every patient (Fig 3). In these images, Reader 1 and 2 were able to identify 11.7±2.8 and 11.7±2.3 anatomical structures per patient on average (out of a total of 13 items), respectively. In comparison, they identified 13±0 and 12.5±0.5 structures per patient from the echography images, respectively. A representative 4-chamber view for both imaging modalities with identified anatomical structures is shown in Fig 4. MR and echo measurements of the diameters showed good agreement for both observers as illustrated by the Bland-Altman (Fig 5a-b) and linear regression (Fig 5c-d) plots. Surface measurements between both modalities yielded similar agreement as for the diameter measurements (Fig 5e). Finally, the intra- and inter-observer variability assessment showed a good overall reproducibility (Fig 5e).Discussion and Conclusion
The qualitative and quantitative results presented in this study validate the use of fetal cardiac MRI as a promising alternative to echocardiography for the assessment of fetal cardiac anatomy and function. The quantitative comparison between the two imaging modalities showed good reproducibility and agreement in terms of diameter and surface measurements. Some of the variability may be explained by the use of slightly different imaging planes for the measurements of diameters and surfaces between each modality. In summary, fetal cardiac cine MRI enables reliable depiction and measurements of anatomical structures of the fetal heart. Further validation of this framework in patients with cardiac pathology is currently ongoing.Acknowledgements
This work was supported in part by the Swiss National Science Foundation grants 320030_143923 and 326030_150828.References
1. Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol 2002;39(12):1890-1900.
2. Gilboa SM, Salemi JL, Nembhard WN, Fixler DE, Correa A. Mortality resulting from congenital heart disease among children and adults in the United States, 1999 to 2006. Circulation 2010;122(22):2254-2263.
3. Quartermain MD, Pasquali SK, Hill KD, Goldberg DJ, Huhta JC, Jacobs JP, Jacobs ML, Kim S, Ungerleider RM. Variation in Prenatal Diagnosis of Congenital Heart Disease in Infants. Pediatrics 2015;136(2):e378-385.
4. Mahle WT, Newburger JW, Matherne GP, Smith FC, Hoke TR, Koppel R, Gidding SS, Beekman RH, 3rd, Grosse SD, American Heart Association Congenital Heart Defects Committee of the Council on Cardiovascular Disease in the Young CoCN, Interdisciplinary Council on Quality of C, Outcomes R, American Academy of Pediatrics Section on C, Cardiac S, Committee on F, Newborn. Role of pulse oximetry in examining newborns for congenital heart disease: a scientific statement from the American Heart Association and American Academy of Pediatrics. Circulation 2009;120(5):447-458.
5. Yerly J, Ginami G, Nordio G, Coristine AJ, Coppo S, Monney P, Stuber M. Coronary endothelial function assessment using self-gated cardiac cine MRI and k-t sparse SENSE. Magn Reson Med 2016;76(5):1443-1454.
6. Chaptinel J, Mivelaz Y, Yerly J, Leonor Alamo L, Prsa M, Vial Y, Gudinchet F, Berchier G, Ledoux JB, Stuber M. A Golden-Angle Acquisition Coupled with k-t Sparse SENSE Reconstruction for Fetal Self Retro-Gated Cine Cardiac MRI: an In Vivo Feasibility Study. 2016; Singapore, Singapore. p 0459.
7. International Society of Ultrasound in O, Gynecology, Carvalho JS, Allan LD, Chaoui R, Copel JA, DeVore GR, Hecher K, Lee W, Munoz H, Paladini D, Tutschek B, Yagel S. ISUOG Practice Guidelines (updated): sonographic screening examination of the fetal heart. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology 2013;41(3):348-359.
Figures