3161
Feasibility Study: 2-D Self-Navigation using Compressed Sensing Reconstruction for Respiratory Gating in Free-breathing 3-D CINE Imaging1Pattern Recognition Lab, Department of Computer Science, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany, 2Erlangen Graduate School in Advanced Optical Technologies (SAOT), Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany, 3Siemens Healthcare GmbH, Magnetic Resonance, Erlangen, Germany, 4Universitätsklinikum Erlangen, Erlangen, Germany
Synopsis
We investigate the feasibility of using 2-D self-navigation for respiratory gating for free-breathing whole-heart 3-D CINE imaging, where respiration-induced cardiac motion may be more easily detected than in commonly used 1-D self-navigation methods. We compare self-navigation images, derived gating signals and resulting 3-D CINE images of the 1-D and 2-D methods and find that respiratory motion can be well visualized with the 2-D method; both methods show a good overlap of gating signals and little difference in resulting image quality. 2-D self-gating may thus be considered a promising alternative to 1-D self-navigation as it allows easier detection of respiratory motion.
Introduction
Common respiratory self-navigation approaches1,2 employed for free-breathing cardiac imaging derive signals for respiratory motion correction from 0-D or 1-D data, e.g., the central k-space point or central k-space line in superior-inferior (SI) direction. While 1-D approaches may capture the main component of respiratory motion, separating respiration-induced motion of the heart from other moving structures in a 1-D signal is challenging. We propose an approach for 2-D respiratory self-navigation based on an undersampled acquisition of self-navigation data and subsequent compressed sensing (CS) reconstruction, applied to a respiratory-gated 3-D CINE scan. In addition to solving the aforementioned problem with 1-D signal interpretation, motion in directions other than SI can be detected as well. We demonstrate the feasibility of this approach in a volunteer experiment and compare against a reference 1-D self-navigation method2.Methods
For 1-D self-navigation, only a single central k-space line needs to be acquired periodically during the imaging process, e.g., once in each heartbeat. For 2-D self-navigation, we use one cardiac phase of the 3-D CINE acquisition in each heartbeat to capture undersampled self-navigation data for sagittal 2-D projection images (see Figure 1). Fully-sampled 2-D navigators have been previously proposed for coronary MRA3. We perform full sampling of a small central k-space region followed by stratified sampling4 with one random sample per stratum in the k-space periphery. The remaining data for 3-D CINE imaging is acquired as previously described2. Note that this acquisition strategy allows a comparison to the 1-D method within the same dataset as the central k-space line is also acquired in each heartbeat.
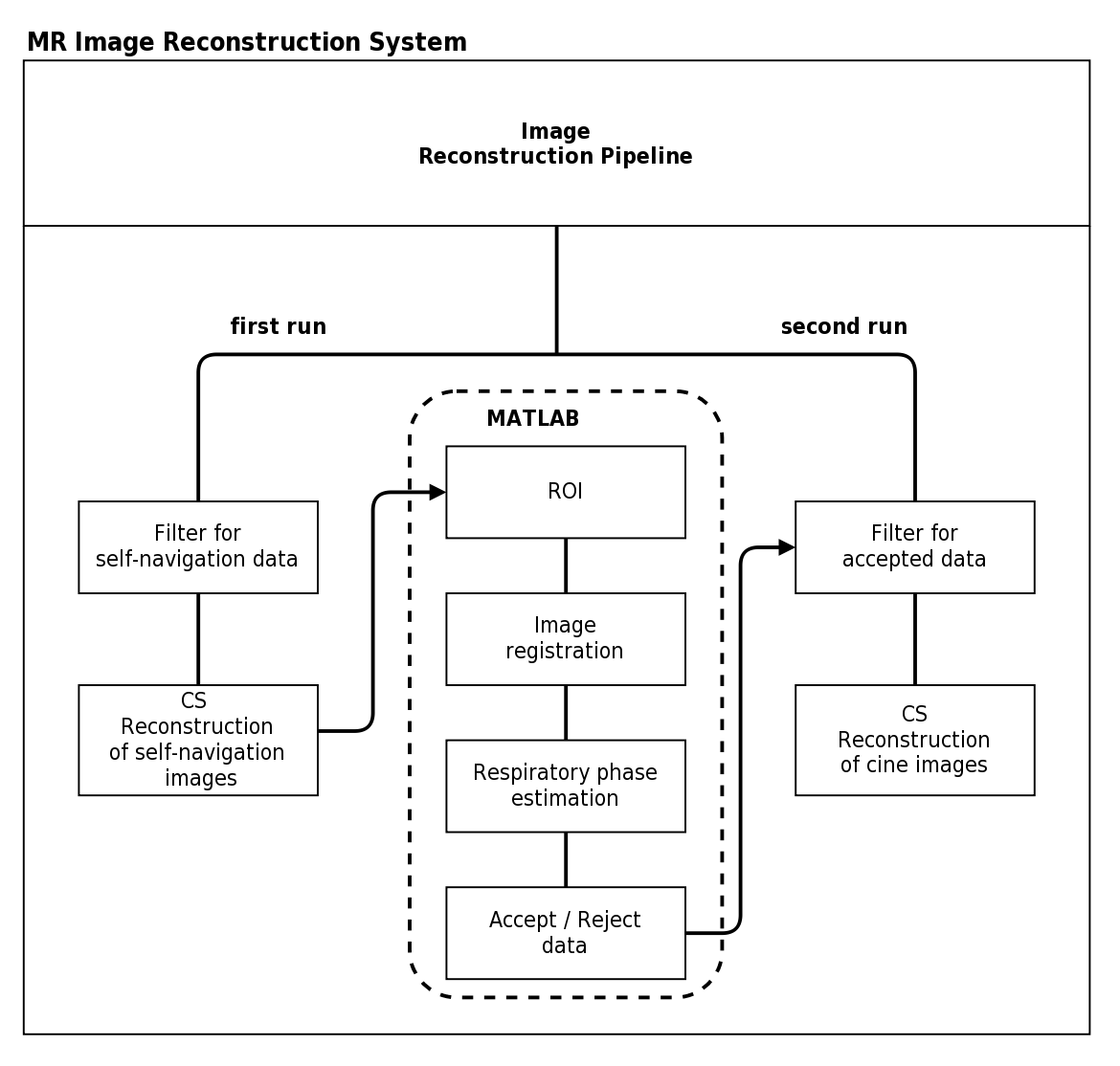
Figure 2 shows a flow chart of the image reconstruction pipeline. The compressed sensing reconstructions for both the intermediate self-navigation images and the final 3-D CINE image were performed as previously described5.
Motion detection in self-navigation images is restricted to a manually selected region of interest over the heart. Pair-wise image registration6 of all self-navigation images to a common reference frame is performed to obtain deformation fields $$$\vec{d}_{k}(x, y)$$$ between the reference frame (manually selected in end-expiration) and the $$$k^\text{th}$$$ self-navigation image. The data of a heartbeat is accepted for the final 3-D CINE reconstruction if the mean magnitude of the deformation field corresponding to its self-navigation image is below a threshold $$$ε$$$: $$\frac{1}{N}\sum_x^{}\sum_y^{}\parallel\vec{d}_{k}(x, y)\parallel_{2} <ε,$$ where $$$N$$$ is the number of pixels in the self-navigation image.
To demonstrate the feasibility of this approach, 3-D CINE imaging was performed in a volunteer (female, age 27) on a 1.5 T clinical MR scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). A volume-selective, ECG-gated bSSFP prototype imaging sequence with the following parameters was used: TR=2.8 ms, TE=1.2 ms, FOV=340x209x209 mm3, voxel size (1.9 mm)3, temporal resolution 42 ms, fixed acceleration factor of 2.6 compared to the fully-sampled matrix (before respiratory gating) for the undersampling of 3-D CINE data, and acceleration factor of 8 for the self-navigation data. For signal reception, 18+12 elements of an anterior+posterior local coil matrix were used.
For evaluation, we compared the 1-D and 2-D self-navigation signals and derived gating results as well as a qualitative comparison of the resulting 3-D CINE images.
Results and Discussion
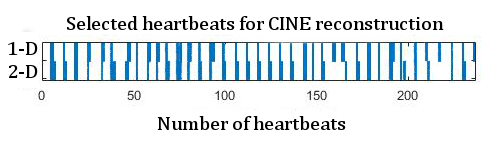
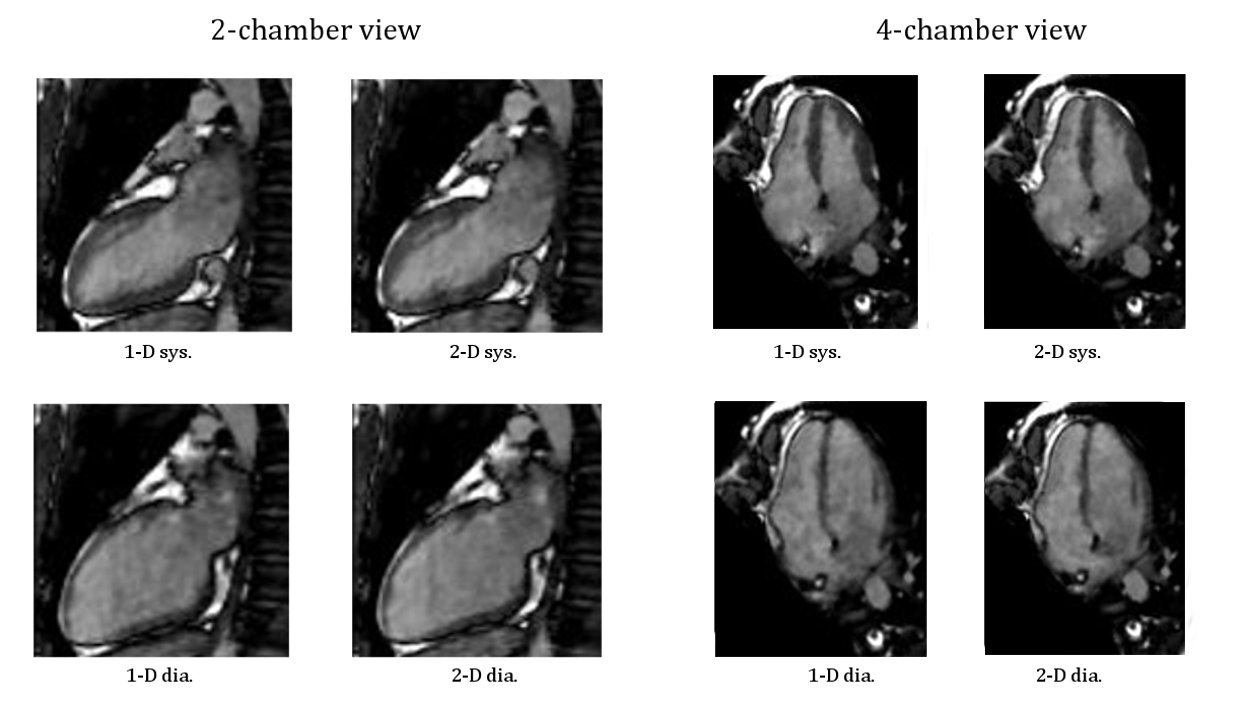
Figure 3 shows the self-navigation images of the 1-D and proposed 2-D approach. The derived gating signals of both methods can be seen in Figure 4 and have an overlap of 81%. A qualitative comparison of the resulting 3-D CINE images is given in Figure 5.
Respiratory motion is clearly observable in the 2-D self-navigation
images. Their advantage is that respiration-induced cardiac motion can be
easily separated from other moving structures, e.g., the chest wall, whereas
they are mixed together in the 1-D signal. The 1-D signal was manually selected
from the choice of 30 receiver coils as the one where respiratory motion is
seen most clearly, which requires an experienced operator. This is not required
for the presented 2-D method. Both methods show a reasonable overlap in derived
gating signals, and the qualitative comparison shows little difference in image
quality. We expect that the 2-D approach can outperform the 1-D method in cases
of complex breathing patterns with uncorrelated respiratory motion in
directions orthogonal to the SI direction. Future work will be the automation
of manual steps and full scanner integration.
Conclusion
We have demonstrated the feasibility of a 2-D self-navigation approach for free-breathing 3-D CINE imaging. The 2-D self-navigation images allow a direct observation of the respiration-induced cardiac motion, which can then be used for respiratory gating or motion correction. In contrast to the commonly used 1-D approach, the respiratory motion can be better characterized and separated from confounding influences.Acknowledgements
The authors gratefully acknowledge funding of the Erlangen Graduate School in Advanced Optical Technologies (SAOT) by the German Research Foundation (DFG) in the framework of the German excellence initiative.References
[1] D. Piccini et al. "Respiratory self-navigation for whole-heart bright-blood coronary MRI: methods for robust isolation and automatic segmentation of the blood pool". Magn. Reson. Med. 68(2):571-9, 2012.
[2] Wetzl, Jens, et al. "Free-Breathing, Self-Navigated Isotropic 3-D CINE Imaging of the Whole Heart Using Cartesian Sampling."
[3] M. Hennigsson et al. "Prospective respiratory motion correction for coronary MR angiography using a 2D image navigator". Magn. Reson. Med. 69(2):486-94, 2013.
[4] C. Särndal et al. “Stratified Sampling”. Springer Publishing, 2003. ISBN 0-387-40620-4.
[5] J. Wetzl et al. "Isotropic 3-D CINE Imaging with Sub-2mm Resolution in a Single Breath-Hold". Proc. ISMRM #1011, 2015.
[6] H. Xue et al. “Motion Compensated Magnetic Resonance Reconstruction Using Inverse-Consistent Deformable Registration: Application to Real-Time Cine Imaging”. MICCAI 2011, pp. 564-572.
Figures
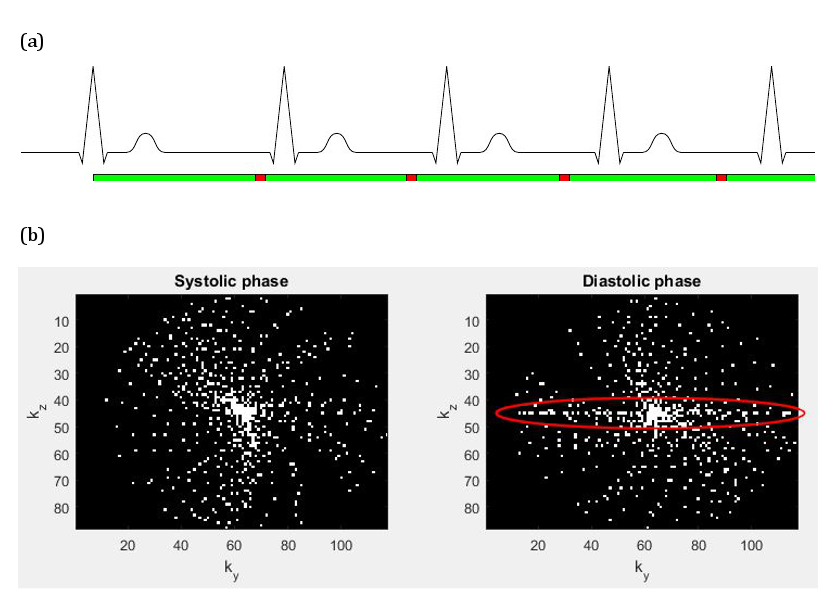
(b) Sampling patterns of a systolic phase (left) with only 3-D CINE data and a diastolic phase (right) with mixed 3-D CINE and self-navigation data (red ellipse) in the kz = 0 plane.