3154
Global circumferential strain derived from feature tracking imaging can detect early subclinical myocardial disorders in patients with heart failure preserved ejection fraction: Comparison with tagged cine magnetic resonance imaging1Department of Radiology, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan, 2Division of Cardiology, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan
Synopsis
The heart failure preserved ejection fraction (HFpEF) accounts for 40–50% of all causes of heart failure. For HFpEF, identification of strain disturbances where systolic function is seemingly preserved is a decisive step toward revealing hidden heart damage. Recently, the novel technique of feature tracking imaging (FTI) was introduced for myocardial strain measurement directly from conventional cine images. We demonstrated that FTI allows for detailed strain assessment with acceptable correlation with the tagging method. In particular, global circumferential strain, which cannot be detected by analysis using cine images, may possibly serve as a sensitive and early marker of cardiac dysfunction.
Introduction
Heart failure preserved ejection fraction (HFpEF) is characterized by symptoms of congestive heart failure, apparently preserved left ventricular (LV) systolic function, and impairment of LV diastolic function.1 HFpEF is of importance as it accounts for 40–50% of all causes of heart failure, and its morbidity and mortality rates are similar to those for heart failure related to systolic dysfunction. The identification of strain disturbance associated with HFpEF when systolic function is seemingly preserved would be a decisive step toward revealing hidden heart damage in many pathologic conditions. Tagged cine magnetic resonance imaging (MRI) has been established as a non-invasive technique for the accurate measurement of myocardial strain. However, additional scans are necessary and the post-processing procedure is time consuming. Feature tracking imaging (FTI), which allows direct derivation of myocardial strain from conventional cine sequences, is a recently introduced novel technique.2Purpose
The aim of this study was to assess the utility of FTI for LV strain assessment in patients with HFpEF and to compare it with tagged cine MRI.Methods
Ten patients with HFpEF and five healthy volunteers underwent cardiac MRI with a 1.5-T scanner (MAGNETOM Sonata, Siemens AG Healthcare Sector, Erlangen, Germany). HFpEF was defined as a clinical history of heart failure (NHYA functional class >II) and apparently preserved LV contraction (LVEF >50% by cine MRI). Short and long axial cine images were obtained by using segmented SSFP (True-FISP) cine sequences with a standardized clinical protocol (TE/TR=1.6/3.2 msec, FOV 340 mm, matrix 190×190, slice thickness 6 mm, and temporal resolution 45 msec). The grid-type tagged cine images with a 6-mm tag spacing were acquired in the short axis plane (TE/TR=2.54/3.2 msec, FOV 340 mm, slice thickness 6 mm, and temporal resolution 35 msec). Myocardial strains were obtained with dedicated feature tracking software (Diogenes MRI, TomTec Imaging Systems, Germany). Following semi-automated tracing of endocardial and epicardial borders on short axis cine images, global radial and circumferential strains (GRS and GCS) were calculated (Figure 1). Tagged cine images were also analyzed with a post processing workstation (Zio station 2 software, Ziosoft Inc., Japan), and then the GRS and GCS were automatically calculated. The strain values acquired from FTI and tagging were compared.Results
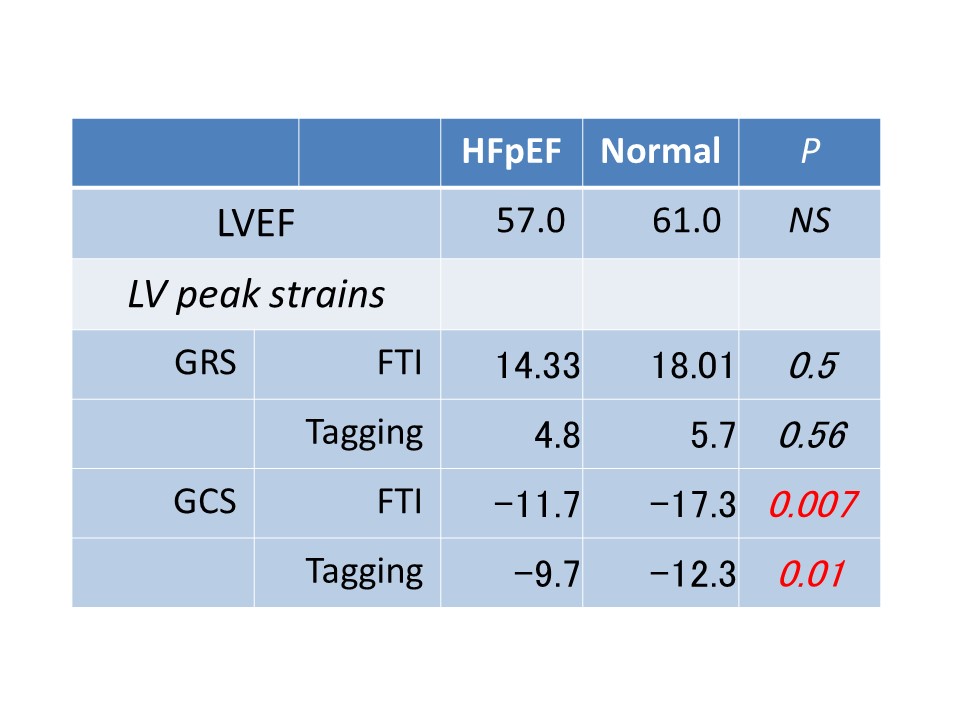
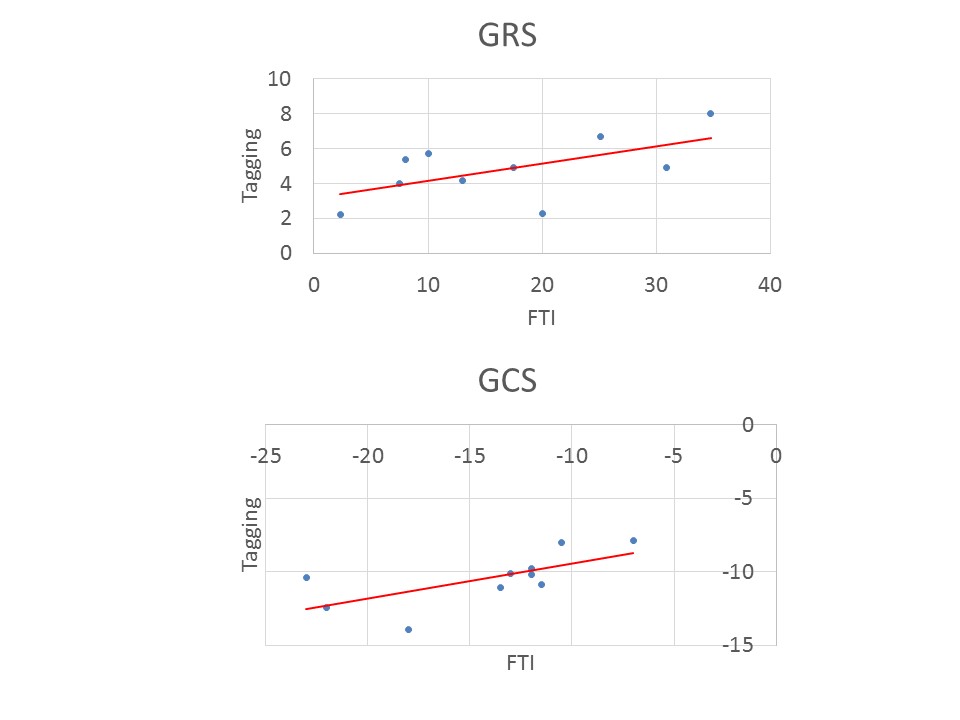
No significant differences were noted in cardiovascular characteristics (heart rate, LV volume, and LVEF) between HFpEF and normal subjects. Table 1 shows the strain values derived from FTI and tagging in HFpEF and normal subjects. In both methods, the GCS was significantly reduced in HFpEF patients when compared with normal subjects (FTI p=0.007, tagging p=0.01), whereas the GRS was lower in HFpEF patients than in normal subjects, but these differences did not reach statistical significance (FTI p=0.50, tagging p=0.56). The GCS obtained from FTI showed good correlation with that obtained from tagging (r=0.81, p=0.02) (Figure 2), while the GRS obtained from FTI showed only modest correlation with that obtained from tagging (r=0.59, p=0.07) (Figure 2). FTI-derived strain values tended to be higher than those obtained with the tagging method.Discussion
Our results demonstrate that FTI allows the detailed assessment of LV strain from conventional cine images and shows acceptable levels of correlation with the tagging method. Strain values were systematically higher when obtained with FTI than with tagging, although this might have been due to the different techniques employed. FTI software delivers outputs of myocardial strain, segmental velocity, and displacement parameters that are relatively quick in terms of image acquisition and post processing. The technique avoids the additional time needed for tissue phase mapping or tagging and raises the possibility of retrospective analysis of existing MRI datasets. Herein, when compared to normal control subjects, GCS measurements were significantly impaired in patients with HFpEF. Previous research has showed that the circumferential fiber shortening in the mid-wall may better reflect intrinsic contractility than radial contraction of fibers in endocardium.3 Despite the preserved systolic function and regional wall thickening, GCS indicated that circumferential fiber shortening was impaired in patients with HFpEF and may serve as a sensitive and early marker of cardiac dysfunction.Conclusion
Myocardial strain measurement using FTI showed good correlation with values obtained with tagged cine MRI and has the potential to detect early subclinical myocardial disorders that cannot be detected by conventional analysis using cine images.Acknowledgements
No acknowledgement found.References
1. Paulus WJ, Tschöpe C, Sanderson JE, et al. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J. 2007;28(20):2539–2550.
2. Augustine D, Lewandowski AJ, Lazdam M, et al. Global and regional left ventricular myocardial deformation measures by magnetic resonance feature tracking in healthy volunteers: comparison with tagging and relevance of gender. J Cardiovasc Magn Reson. 2013;15:8.
3. Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18(12):1440–1463.
Figures