3146
Quantitative Evaluation of Ultra-fast Real Time Imaging Compared to Cine at 1.5 T and Demonstration of Clinical Value in Atrial Fibrillation1OCMR, Oxford University, Oxford, United Kingdom, 2RDM, Oxford University, Oxford, United Kingdom, 3Biomedizinishe NMR Forschungs GmbH, Max-Plank-Institut fur biophysikalische Chemie, Gottingen, Germany
Synopsis
Ultra-fast real time imaging allows cine imaging of the whole heart without gating or breath-holding in around 1 minute. Here clinical cardiac metrics are evaluated and compared with those from a standard clinical acquisition in normal volunteers. We find agreement adequate for clinical use. The real time approach is evaluated in a case of atrial fibrillation and found to provide a more robust evaluation of cardiac parameters in a shorter acquisition time.
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia characterized by irregular and often rapid ventricular rate. Assessment of cardiac function in patients with AF using Magnetic Resonance Imaging (MRI) is challenging due to poor image quality often necessitating frequent repeat acquisitions. Breath-held (BH) ECG gated balanced steady state free precession (bSSFP) cine is currently the mainstay in clinical cardiac assessment of biventricular function. Image quality is often compromised by patient’s cardiac rhythm and capacity to breath-hold. Recent advances in methodology have made real time (RT) cardiovascular magnetic resonance (CMR) imaging possible removing the requirement for ECG synchronization and for breath-holding [1,2]. Whilst high quality RT results have been shown, the inter-observer variability and systematic differences between these two methods have not previously been studied. We therefore sought to determine the level of agreement between an ultra-fast real time free breathing 1 min short-axis (SA) sequence and a standardized BH retro gated ECG bSSFP cine. Subsequently this approach was used to compare the results of cardiac mass and function assessment using standard prospective cine steady state free precession (SSFP) and radial RT imaging in a patient with persistent AF with variable ventricular rate.Methods
10 healthy volunteers were scanned on a 1.5 T Avanto-Fit Siemens MR scanner equipped with a radial RT pulse sequence [1] and a high performance online image reconstruction computer (GPU server) equipped with algorithms supplied by the Max-Planck-Institut für biophysikalische Chemie, Göttingen, Germany [1]. Whole heart short axis stack was acquired with matched protocols (1) standard BH cine requiring 8-11 breath-holds and (2) free breathing ECG-free RT with a duration of 1 min for 15 slices (4s per slice). Scan parameters included slice thickness of 8mm with no gap, nominal temporal resolution of 33 ms for RT and 40 ms for cine, pixel sizes were 1.6x1.6mm2 for RT and 1.4x1.4 mm2 for cine, TR/TE were 3.04/1.53ms and 3.00/1.14ms for RT and cine respectively. Two blinded, clinically experienced CMR observers independently analyzed cardiac mass, chamber volumes and ejection fraction (EF) on bSSFP cine and RT imaging using a standard software package (cvi42 version 5.3.4, Circle Cardiovascular Imaging Inc). The real-time analyses of EF, volumes and chamber size mirrored routine echocardiographic assessment of cardiac function and therefore restricted to 1 heart beat with no discrimination of respiratory phase. A 62-year-old male patient with persistent AF and rapid ventricular response (90-115 bpm) was evaluated replicating the above methodology. All data acquisition and analyses followed our institutional guidelines.Results
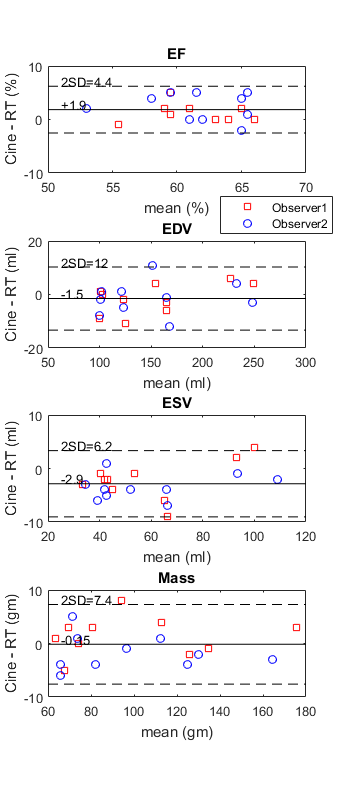
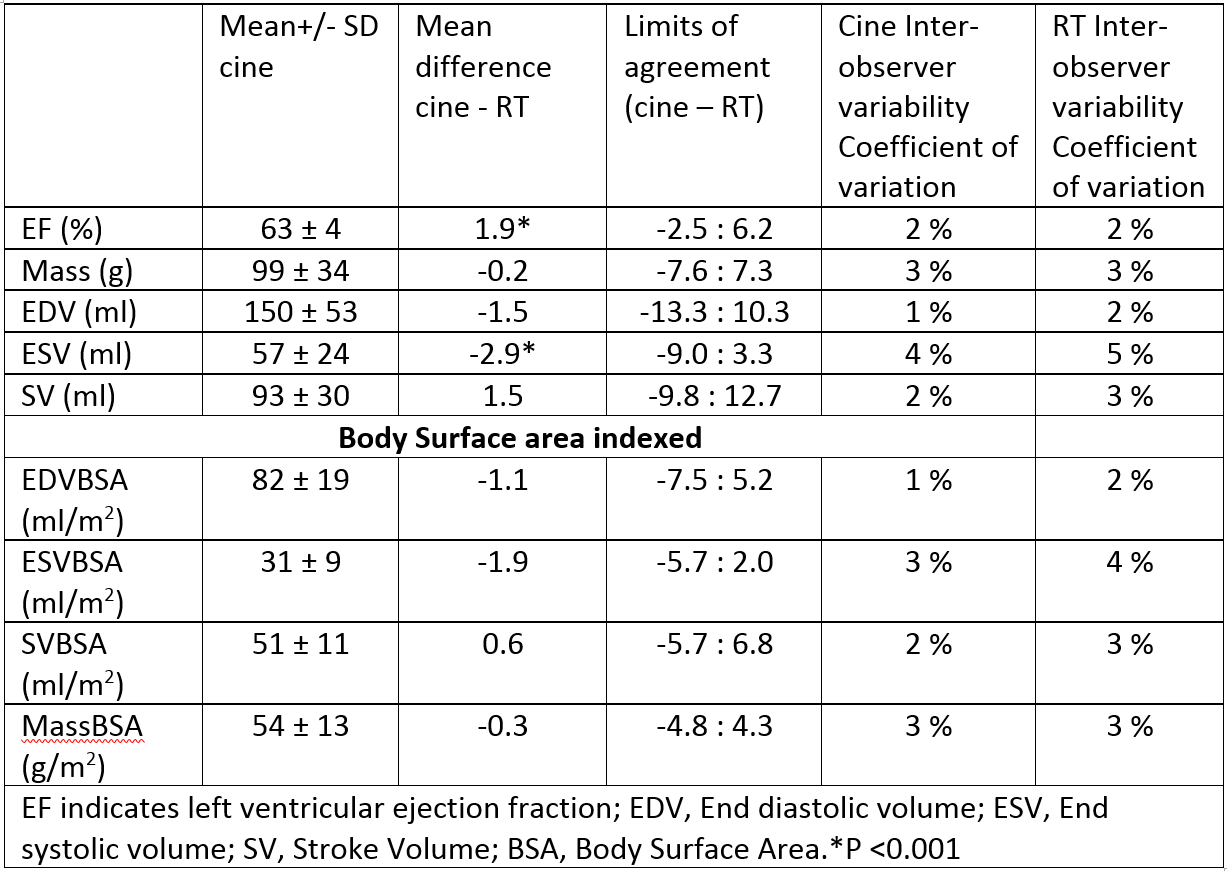
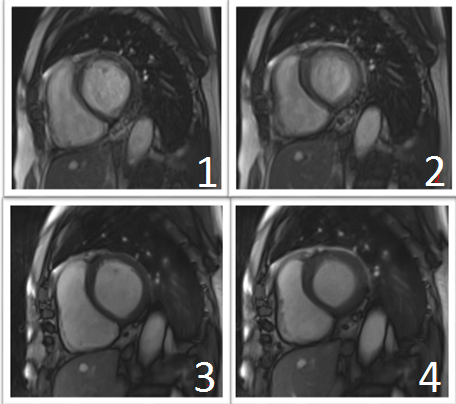
Images were of good quality for both acquisition schemes. The inter-observer variability was similar for both RT and cine for all volume and mass parameters (Figure 1). The limits of agreement were within 10% for all measures with no significant differences (paired t-test) except those relating to systolic volume (Figure 2) that was marginally higher resulting in lower EF. Despite this, the limits of agreement for EF were -2.5% to 6.2% and considered to be clinically acceptable. In the patient example, time to acquire the prospectively gated cine with repeated attempts to optimise image quality was 5 minutes for BH cine versus 2 minutes for RT imaging. Image quality of prospectively triggered loop was impaired in comparison to RT (Figure 3). Left ventricular EF was markedly lower on analysis of prospectively triggered cine loop at 24% compared to 40% on RT imaging. End-diastolic volume (EDV) and stroke volume (SV) were higher in RT than on standard cine with a difference of 14% and 49%, respectively. End-systolic volume (ESV) and mass were similar with a difference of only -7% and 1%, respectively.Discussion
This work provides preliminary quantitative validation of RT CMR for determining the evaluation of EF, cardiac mass and chamber volumes using standard processing tools. The RT method is particularly valuable in cases where a standard cardiac gated breath-held acquisition doesn’t work (e.g. unable to breath-hold, unable to communicate breath-hold instructions, failure to gate, gating irregularities) and provides complete coverage of the heart much quicker than the standard breath-held approach.Conclusion
With comparable diagnostic image quality to BH cine, RT imaging offers the potential for fast, reliable, ECG-free, non-breath hold cardiac assessment of left ventricular volumes, mass and EF over several heart beats in 2 minutes. This approach appears to satisfactorily address a real clinical need in the evaluation of cardiac function in patients with AF.Acknowledgements
The authors thank the BHF, Oxford NIHR and MRC for supporting this work.References
1) S. Zhang, A.A. Joseph, D. Voit, S. Schaetz, K-D. Merbolt, C. Unterberg-Buchwald, A.Hennemuth, J. Lotz, J. Frahm. Real-time magnetic resonance imaging of cardiac function and flow-recent progress. QIMS 2014, 4(5):313-329
2) Bauer RW, Radtke I, Block KT, Larson MC, Kerl JM, Hammersting lR, et al. True real-time cardiac MRI in free breathing without ECG synchronization using a novel sequence with radial k-space sampling and balanced SSFP contrast mode. The International Journal of Cardiovascular Imaging. 2013;29(5):1059-67.
Figures