3138
Single-Shot Coronary QISS MRA in Children using Radial k-Space Sampling and Compressed Sensing1Biomedical Engineering, Northwestern University, Chicago, IL, United States, 2Department of Radiology, NorthShore University HealthSystem, Evanston, IL, United States, 3Department of Radiology, Northwestern University, Chicago, IL, United States, 4Cardiovascular MR R&D, Siemens Healthineers, Chicago, IL, United States
Synopsis
Coronary MRA is complex to set up (e.g., navigator gating to track respiratory motion), typically takes 5-10 min to complete, and often produces inconsistent results. Quiescent-Interval Slice-Selective (QISS) MRA is a promising method for rapid coronary imaging. We sought to develop a single-shot (real-time) coronary QISS MRA using compressed sensing.
Introduction
Despite the progress made with coronary MRA1, it remains inferior to CT angiography (CTA). Coronary MRA is complex to set up (e.g., navigator gating to track respiratory motion), typically takes 5-10 min to complete, and often produces inconsistent results. In children, coronary MRA is needed for evaluation of origins and is conducted with administration of a gadolinium-based contrast agent and general anesthesia, both of which add health risk and cost. Coronary Quiescent-Interval Slice-Selective (QISS) MRA2 with radial k-space sampling was recently developed to produce high quality images in a single breath-hold of 20 s. This rapid method for coronary MRA does not require contrast agent administration and can be repeated as needed to produce diagnostically acceptable image quality. We sought to develop a single-shot coronary QISS MRA pulse sequence using compressed sensing3, in order to enable free-breathing scanning in children.Methods
Pulse Sequence: A prototype of two-shot coronary QISS MRA was implemented on a 1.5T scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). Relevant imaging parameters include: FOV of 180 mm × 180mm, matrix size of 128 × 128, slice thickness of 2.1 mm, 96 rays (48 rays per heart beat) with 13.123° increments, flip angle 140°, TE = 1.9 ms, TR = 736 ms, echo spacing (ESP) = 3.7 ms, inversion time (TI) = 650 ms. We imaged 16 pediatric patients (mean age = 16.6 ± 8.5 years; 9 males; 7 females) undergoing clinical cardiovascular MRI. The study was approved by the local ethics board, and informed consent was obtained from all participants (or parents in case of minors).
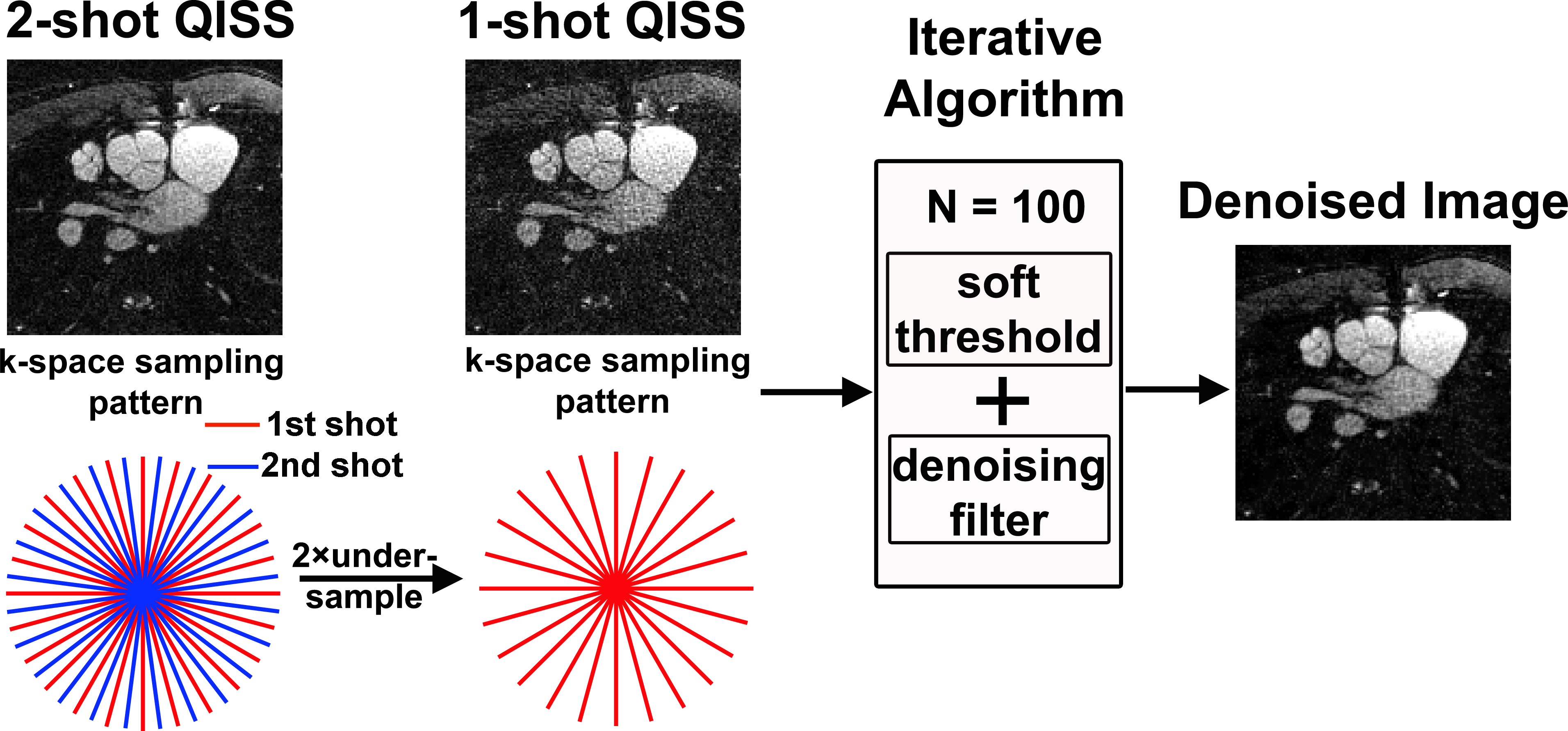
Image Reconstruction: Two-shot QISS data were retrospectively undersampled by a factor of two and reconstructed using compressed sensing (CS) in a SENSE framework with nonuniform fast Fourier transform (NUFFT). We tested two different sparsifying transforms (denoising methods) : (i) non-local means (NLM)4 and (ii) spatial total variation (TV)3. We used a soft threshold of 2% of the maximum signal intensity as a pre-processing step in iterative denoising algorithms. Reconstructions were done in MATLAB software.
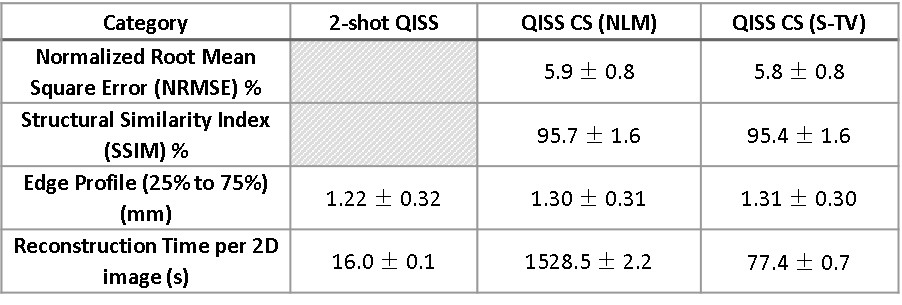
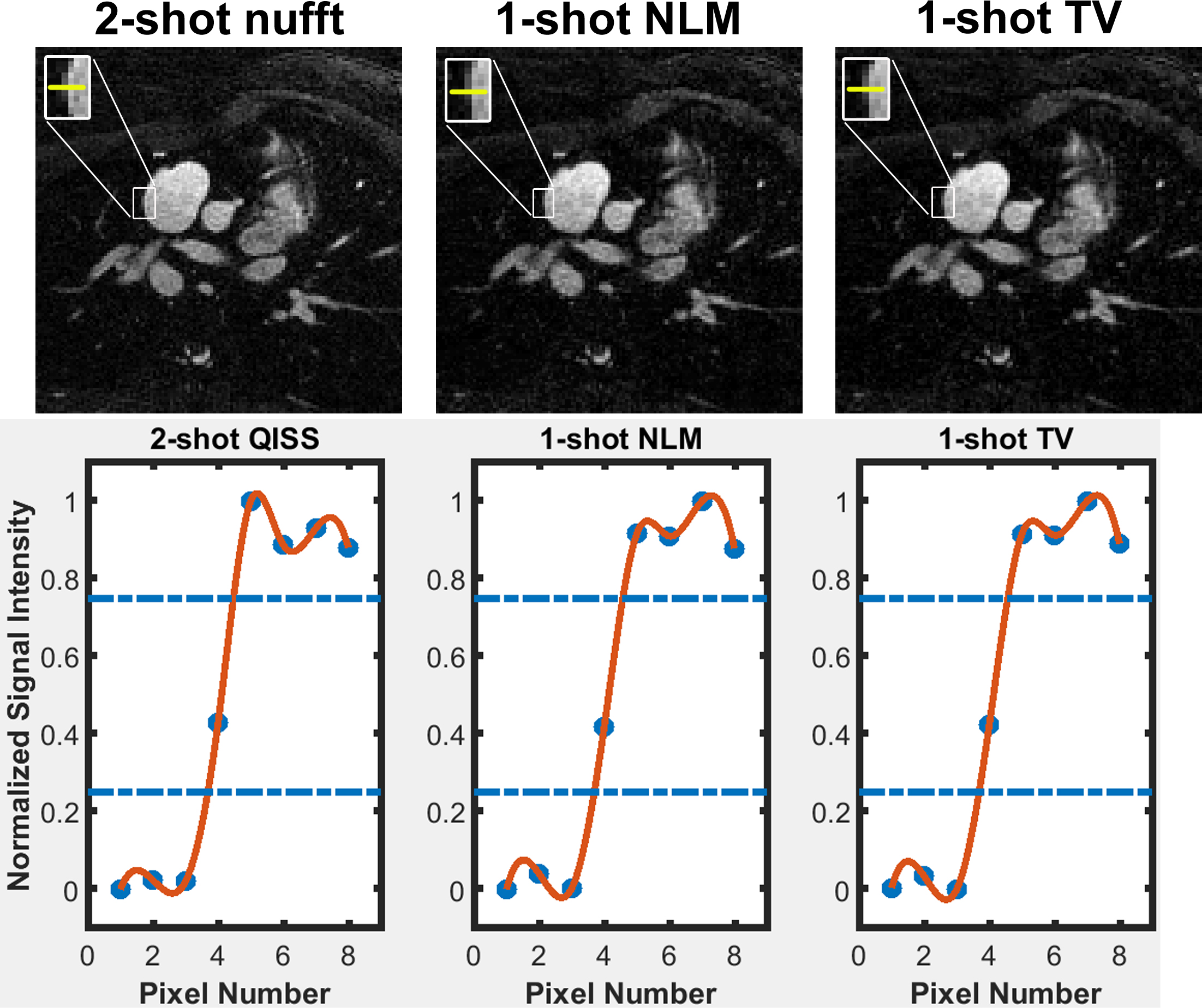
Quantitative Measurements: With two-shot QISS MRA as the reference, we calculated structural similarity index (SSIM), normalized root mean square error (NRMSE) and edge profiles to infer data fidelity. For SSIM and NRMSE calculations, we used a mask to exclude signal-free pixels. For edge sharpness estimation, we measured intensity profiles through an aorta or atrium to background. To increase precision, we interpolated each profile by a factor of 20 and measured the spatial distance between 25 percentiles and 75 percentiles of peak intensity value. We also computed the computation time for each iterative reconstruction algorithm. Quantitative metrics of three groups (2-shot, 1-shot with NLM, 1-shot with TV) were compared using ANOVA, where Bonferroni correction was used to compare each pair (p <0.05 was considered statistically significant).
Results
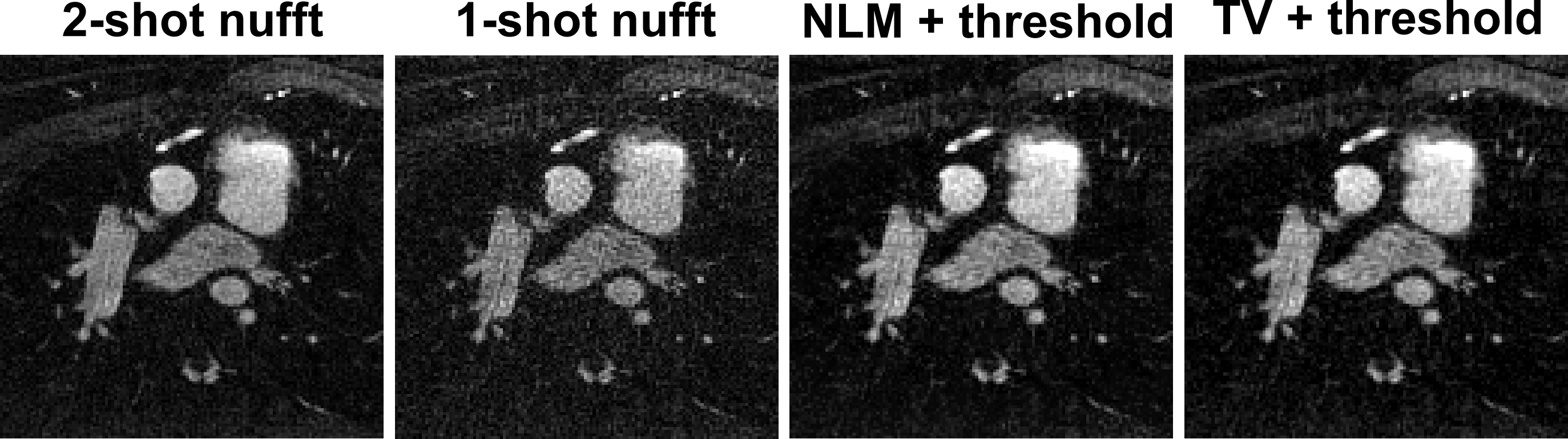
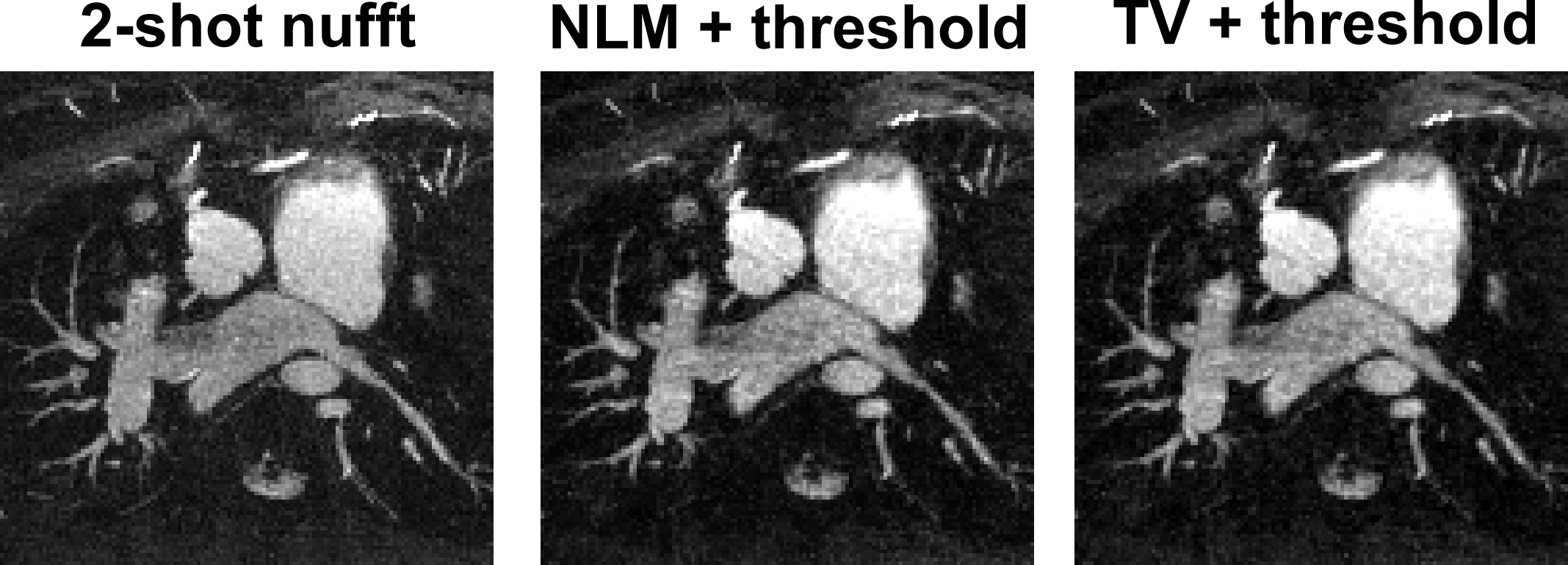
Figure 1 summarizes the overall process of single-shot QISS reconstruction. Figure 2 shows representative images comparing 2-shot QISS, 1-shot QISS with zero padding, 1-shot QISS with NLM denoising, and 1-shot QISS with TV. As shown, 1-shot images with denoising approximate the corresponding 2-shot image. Figure 3 shows representative edge profiles, which show that undersampled QISS images did not produce significant blurring (p = 0.68 > 0.05). Quantitative metrics summarized in Table 1 suggest high data fidelity for both NLM and spatial TV denoising regularization algorithms, whereas the reconstruction time for NLM was significantly higher than spatial TV (p <0.05). Figure 4 shows representative maximum-intensity-projections (MIPs) comparing 2-shot QISS, 1-shot QISS with NLM denoising, and 1-shot QISS with TV.Discussions
This study demonstrates that it is feasible to perform single-shot coronary QISS MRA in children using CS as a denoising filter. While both NLM and spatial TV produced high quality results, spatial TV may be preferred for clinical translation with inline image reconstruction. A future study is warranted to evaluate whether single-shot, free-breathing coronary QISS MRA with motion correction (e.g., diffeomorphic transformations5) during post-processing produces diagnostically acceptable image quality in a diverse set of pediatric patients.Acknowledgements
This work was supported in part by the following grants:
NIH - 1R01HL116895-01A1
References
1. Kim WY, Danias PG, Stuber M, Flamm SD, Plein S, Nagel E, Langerak SE, Weber OM, Pedersen EM, Schmidt M, Botnar RM and Manning WJ. Coronary Magnetic Resonance Angiography for the Detection of Coronary Stenoses. New England Journal of Medicine. 2001;345:1863-1869.
2. Edelman RR, Giri S, Pursnani A, Botelho MPF, Li W and Koktzoglou I. Breath-hold imaging of the coronary arteries using Quiescent-Interval Slice-Selective (QISS) magnetic resonance angiography: pilot study at 1.5 Tesla and 3 Tesla. Journal of Cardiovascular Magnetic Resonance. 2015;17:101.
3. Lustig M, Donoho D and Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magnetic Resonance in Medicine. 2007;58:1182-95.
4. Buades A, Coll B and Morel JM. A non-local algorithm for image denoising. 2005 IEEE Computer Society Conference on Computer Vision and Pattern Recognition (CVPR'05). 2005;2:60-65 vol. 2.
5. Avants BB, Epstein CL, Grossman M and Gee JC. Symmetric diffeomorphic image registration with cross-correlation: evaluating automated labeling of elderly and neurodegenerative brain. Medical image analysis. 2008;12:26-41.
Figures