3136
Dual-Phase Whole-Heart Imaging Using Image Navigation in Congenital Heart Disease1Pediatric Cardiology, UT Southwestern Medical Center Dallas, Dallas, TX, United States, 2Pediatric Cardiology, Children's Health, Children's Medical Center Dallas, Dallas, TX, United States, 3Division of Imaging Sciences, King's College London
Synopsis
Dual phase whole heart imaging allows accurate depiction of cardiac segmental anatomy for congenital heart disease. We applied image-based navigation (iNAV) to improve its clinical utility. Qualitative and quantitative image quality scoring showed that iNAV gave equivalent image quality compared to the standard respiratory navigator. However, the distal coronary arteries were better visualized and the sequence duration was shorter. Using dual-phase iNAV, complete segmental anatomy was delineated in 27/30 patients (90%). The use of iNAV dual phase 3D SSFP whole heart acquisition allows complete morphological diagnosis for congenital heart disease with high image quality with more clinically acceptable time constraints.
Introduction
Dual phase 3D steady-state free precession (SSFP) whole heart acquisition allows simultaneous imaging during both systolic and diastolic rest periods. It has been shown to be accurate in the setting of congenital heart disease to demonstrate segmental anatomy.1 This sequence employs respiratory navigator gating and tracking of the diaphragm, however has limited accuracy due to the estimated factor used to correct cardiac motion with respect to the diaphragm. Further, with typical efficiency of 30-40%, prolonged scanning time is common. In cases of erratic breathing pattern, this navigator may also fail.
An image-navigator (iNAV) has been described which directly tracks the translational respiratory movement of the heart itself in two dimensions2,3. Recent application of image based navigation has been shown to be feasible in single phase whole heart imaging2,3. We sought to apply this technology to the dual phase sequence to evaluate its diagnostic ability in pediatric patients with heart disease.
Methods
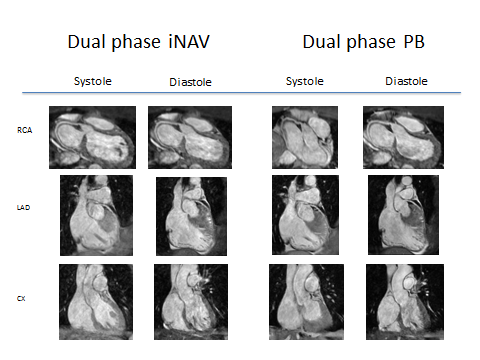
Patients undergoing a clinically indicated cardiac MRI for congenital or pediatric heart disease were included in the study. IRB approval was granted and all subjects were consented. Subjects underwent dual-phase whole heart imaging using both the diaphragmatic 1D pencil beam navigator (PB) and iNAV. The CMRA sequence had the following imaging parameters: FOV=300×300×100mm (coronal orientation), Δx=1.5×1.5×1.5mm3, α=70°, SENSE=2.5 (phase encoding direction). All experiments were performed on a 1.5T clinical scanner (Philips Healthcare, Best, The Netherland) using a 32-channel cardiac coil. The PB Navigator used a gating window of 7mm and 0.6 tracking factor. For the iNAV, separate iNAV references (defined as the first acquired iNAV in each cardiac phase) were acquired for the systolic and diastolic phase. Each subsequent iNAV for a certain phase was registered to its corresponding iNAV reference using normalized cross-correlation. Translational motion correction was performed in foot-head and left-right direction. Additionally, respiratory gating was implemented using the diminishing variance algorithm, assuming a gating efficiency of 50%. The iNAV motion correction and gating was implemented inline on the scanner. Acquisition time was recorded for each sequence and image quality assessed both quantitatively and qualitatively. The dual phase CMRA datasets were reformatted using dedicated software (Soapbubble software tool (Release 5.1 for PRIDE, Philips Healthcare, Best The Netherlands)) to visualize the right coronary artery (RCA), left anterior descending artery (LAD) and the circumflex artery (CX). Vessel sharpness and visualized length were measured for the RCA, LAD and CX for both cardiac phases and for both navigation methods. Qualitative analysis was performed using a previously described and validated visual score2,4 on reformatted images (Figure 1) of each coronary artery in a blinded and randomized fashion by two readers (A.D. and A.T, both with experience in cardiovascular MR imaging) and analyzed using a mixed effect model.Results
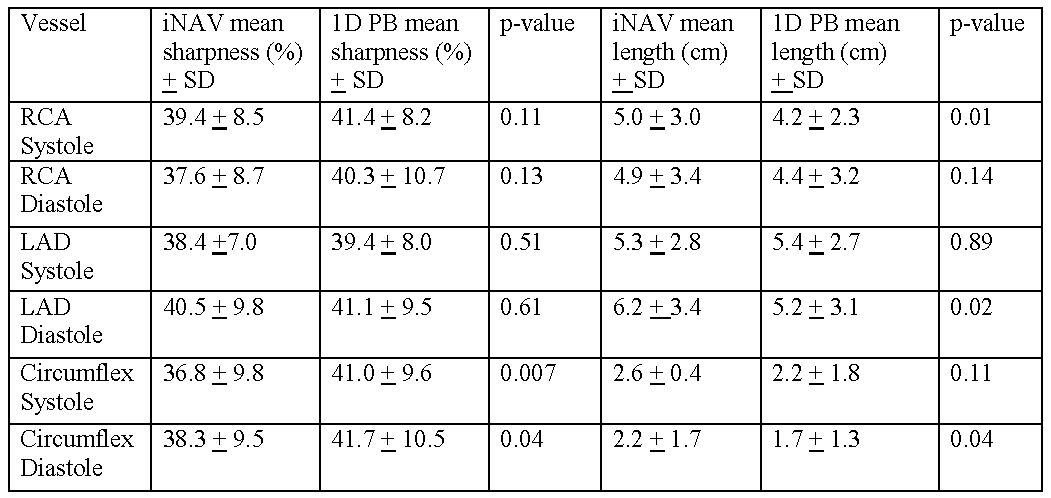
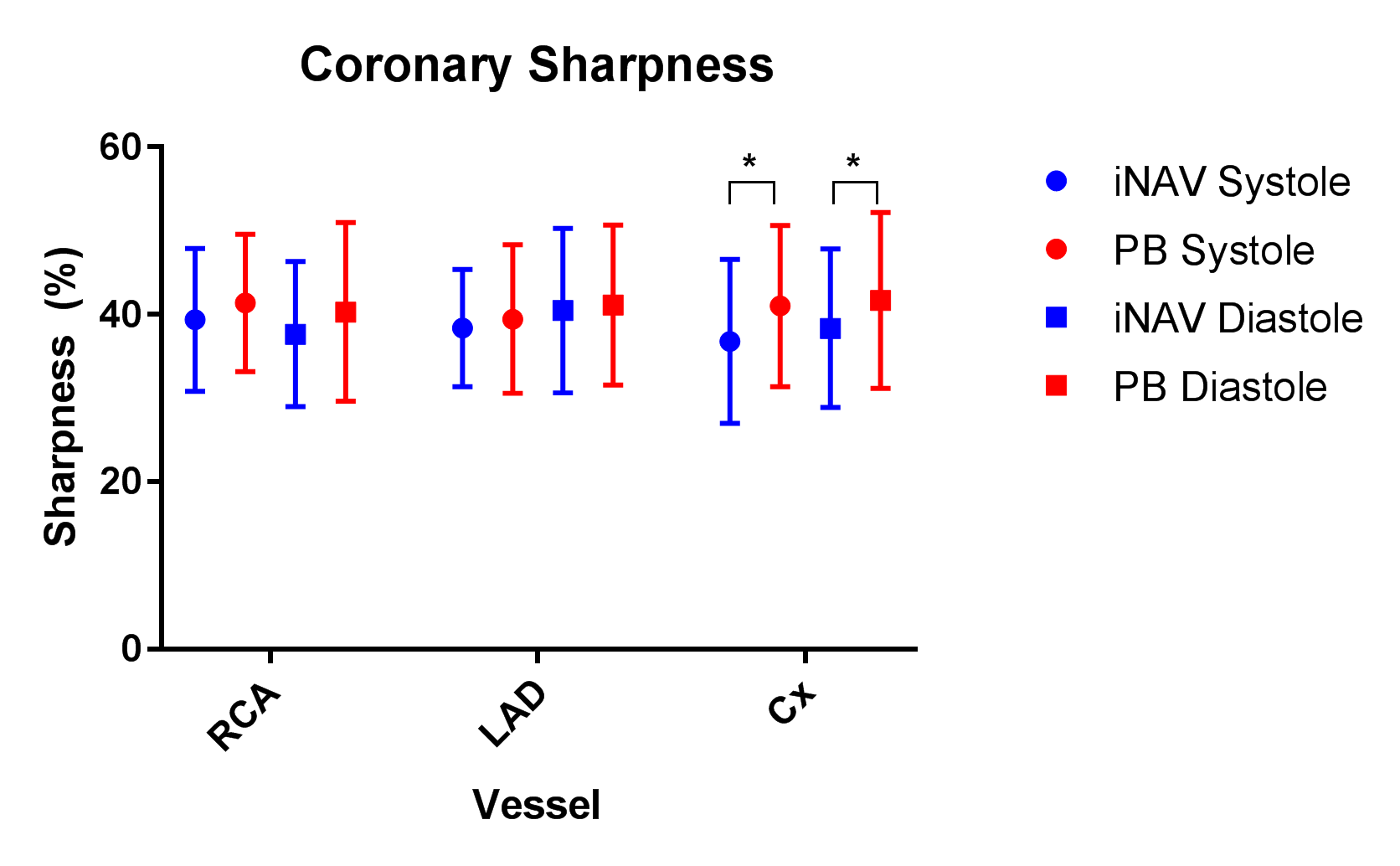
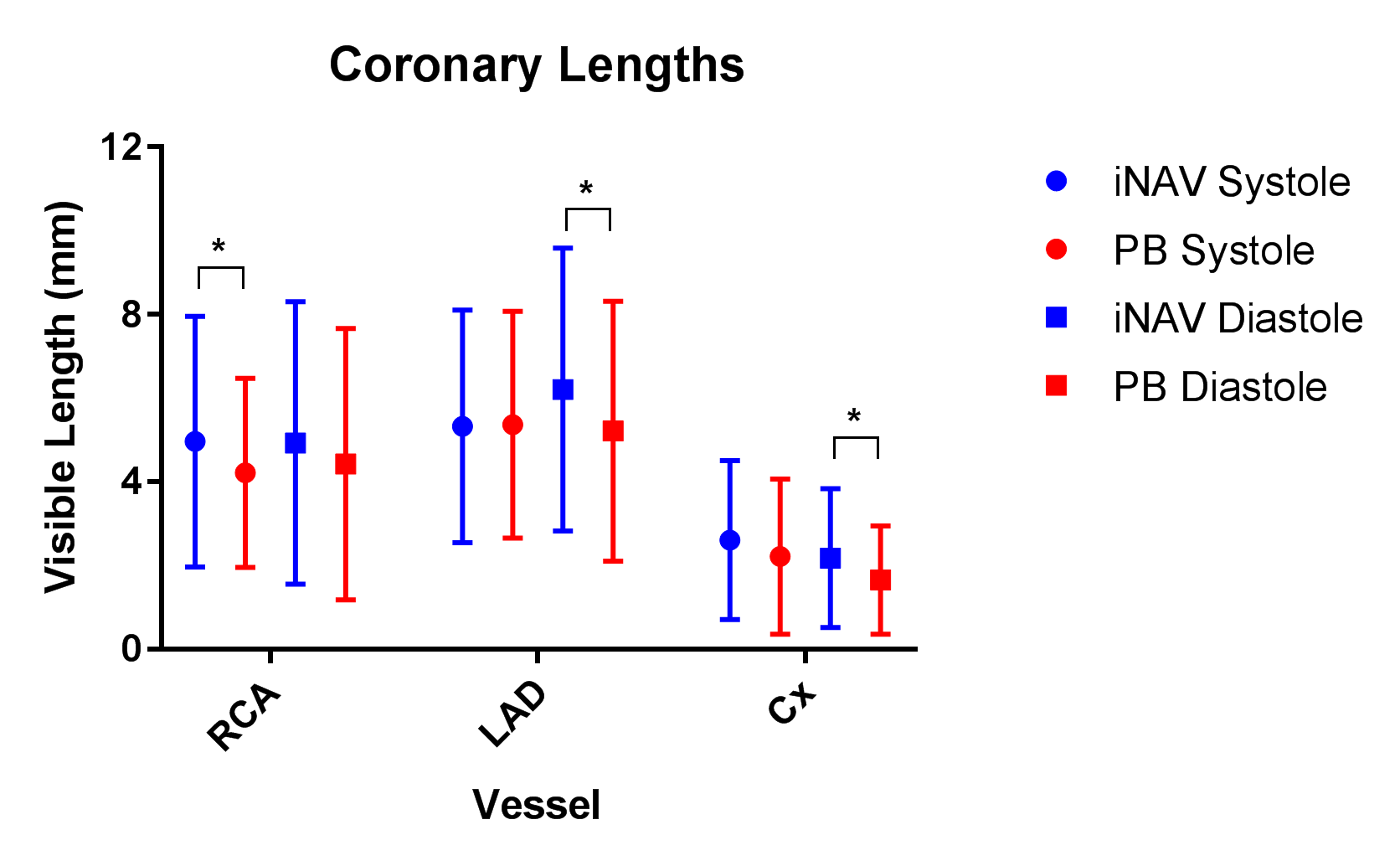
Thirty-two patients underwent 3D dual phase imaging. Two patients failed PB imaging due to erratic breathing patterns and were excluded from analysis. In reviewing quantitative image quality, vessel sharpness was the same for the LAD and RCA in both systole and diastole between the two modalities (Figures 2 and 3). Circumflex sharpness was statistically higher with PB for both systole and diastole (Figures 2 and 3). However, visualized length was greater with iNAV for circumflex in diastole, the LAD in diastole and the RCA in systole (Figures 2 and 4).
There was no statistically significant effect on qualitative image score according to the type of respiratory motion compensation (p = 0.7144).
In assessing cardiac anatomy, iNAV allowed complete morphological diagnosis in 27/30 patients: there were two failures due to an inability in visualizing the right subclavian artery and one failure due to inability to visualize the left upper pulmonary vein.
In evaluating acquisition time, the dual phase CMRA mean scan time was 6 minutes 41 seconds (+/- 2 min 17 sec) using iNAV and 9 minutes 57 seconds (+/- 3 min 29 sec) using PB, a difference that was statistically significant (p = 0.0001).
Discussion
Image quality between iNAV and PB was similar overall with a tendency towards being able to image more of the distal vessel with iNAV. The time needed for image acquisition using iNAV, however, was significantly shorter. As with previous experience with dual phase whole heart imaging, a complete cardiac morphological diagnosis was possible in the vast majority of cases. The shortened acquisition time will significantly improve clinical applicability and patient comfort.Conclusion
The use of iNAV dual phase 3D SSFP whole heart acquisition allows complete morphological diagnosis for congenital and pediatric heart disease with high image quality and with more favorable and clinically acceptable time constraints.Acknowledgements
No acknowledgement found.References
1. Hussain, T., et al., Three-dimensional dual-phase whole-heart MR imaging: clinical implications for congenital heart disease. Radiology, 2012. 263(2): p. 547-54.
2. Henningsson, M., et al., Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med, 2012. 67(2): p. 437-45.
3. Henningsson, M., et al., Prospective respiratory motion correction for coronary MR angiography using a 2D image navigator. Magn Reson Med, 2013. 69(2): p. 486-94.
4. McConnell, M.V., et al., Comparison of respiratory suppression methods and navigator locations for MR coronary angiography. AJR Am J Roentgenol, 1997. 168(5): p. 1369-75.
5. Uribe, S., et al., Congenital heart disease in children: coronary MR angiography during systole and diastole with dual cardiac phase whole-heart imaging. Radiology, 2011. 260(1): p. 232-40.
6. Uribe, S., et al., Volumetric cardiac quantification by using 3D dual-phase whole-heart MR imaging. Radiology, 2008. 248(2): p. 606-14.
Figures