3129
A novel method for performing percutaneous transluminal renal angioplasty with the guide of non-contrast magnetic resonance angiography overlaid on fluoroscopy images1Department of Radiology, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan
Synopsis
Herein, we present a new method for the performance of percutaneous transluminal renal angioplasty (PTRA) guided by non-contrast magnetic resonance angiography (NATIVE True FISP) overlaid on intra-procedural fluoroscopy images. This novel overlay system led to sufficient visualization as the overlaid vasculature on the live fluoroscopic image, and enabled the safe completion of PTRA with fewer angiographic procedures, thus requiring lower volumes of iodinated contrast material and shorter fluoroscopic times.
Introduction
Percutaneous transluminal renal angioplasty (PTRA) has been widely performed for patients with atherosclerotic renal artery stenosis. However, such patients often have a compromised renal function and are therefore at higher risk of complications when receiving iodinated contrast materials during the PTRA procedure. Recently, non-contrast magnetic resonance angiography (MRA) was used as an alternative method to gadolinium-enhanced MRA, proving useful for the evaluation of renal arterial stenosis.1,2
Purpose
Herein, a new method for performing PTRA with the guide of non-contrast MRA overlaid on intra-procedural fluoroscopy images is presented.Methods
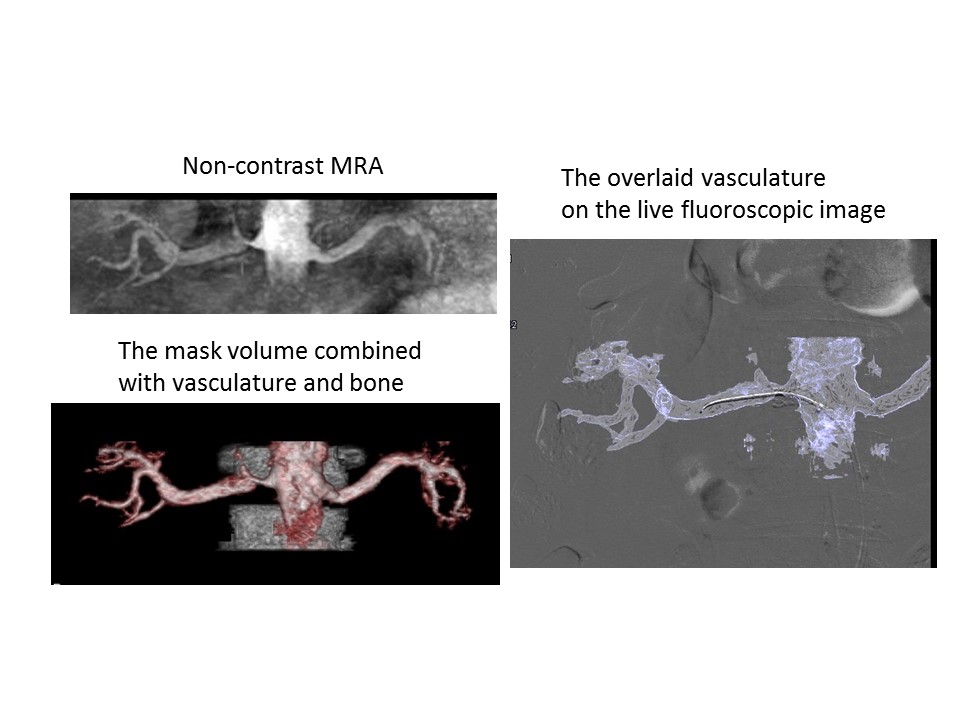
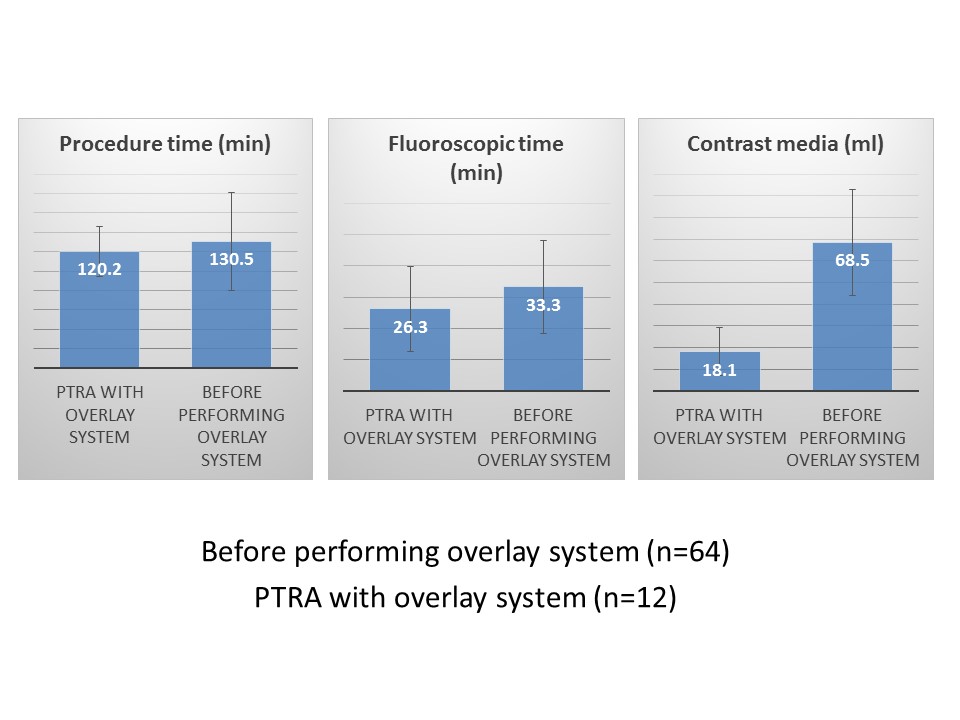
A total of 12 patients scheduled for PTRA were included. Non-contrast MRA was obtained using a respiratory-gated 3D-SSFP proprietary sequence (NATIVE-True FISP, Siemens Healthcare, Germany; imaging parameters: slice thickness 1.0 mm, FOV 340 mm, TR ~1500 msec, TE 1.7 msec, TI 1200–1800 msec, FA 120°, voxel size 1.1x1.1x1.0 mm, data window duration 128–196 msec, and slab 10–12 cm) on a 3-T clinical scanner (MAGNETOM Verio, Siemens Healthcare, Germany). In this sequence, vessel opacification is dependent on an in-flow phenomenon after preparation of the imaging volume with an inversion recovery pulse. The pre-acquired MRA data was used as an “overlay system” and roadmap for navigation3 during the PTRA procedures (Phillips Healthcare, The Netherlands). The mask volume combined with vasculature and bone obtained by non-contrast MRA imaging was registered on fluoroscopic images to mark the lumbar vertebrae as landmarks, and the overlaid vasculature on the live fluoroscopic image was used as a roadmap for navigation during the PTRA procedure (Figure 1). The accuracy of the position of the renal artery origin according to aortography and the procedure time, fluoroscopic time, and amount of contrast media were evaluated and compared with patient data before performance of the overlay system (64 patients).Results
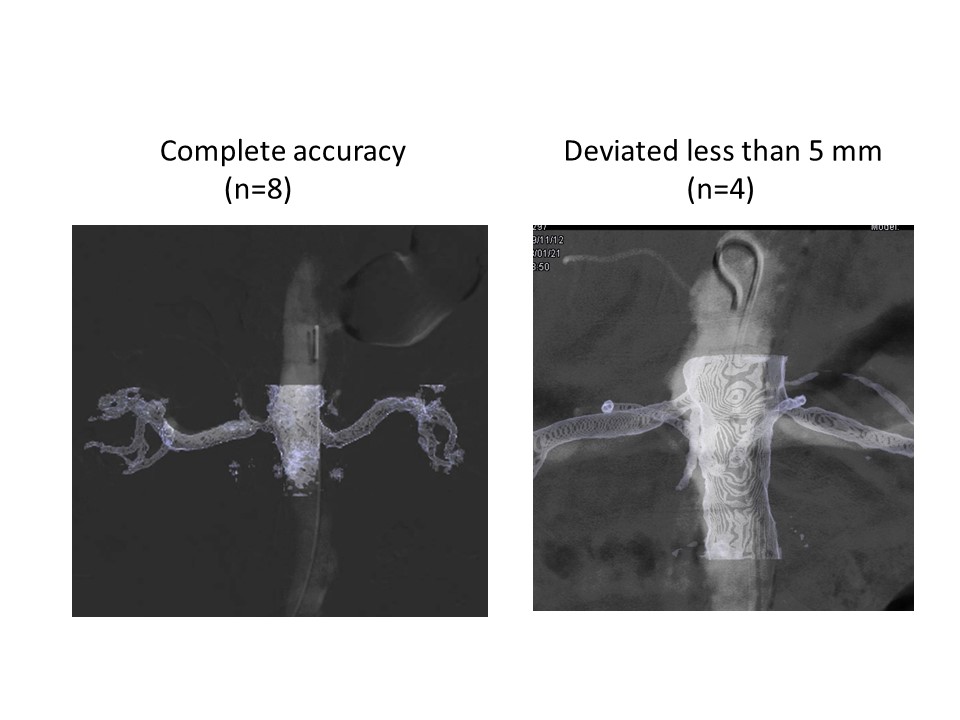
Non-contrast MRA clearly visualized the origin and course of the renal arteries and detected the 13 significant stenoses (assessed by MIP and MPR, visually >50% of lumen narrowing) in 12 patients (one with bilateral stenosis). Mean scan time was 8 min 28 sec. There was good agreement between MRA and digital subtraction angiography in all cases. According to the initial aortography, the origin of the renal artery was registered with complete accuracy in eight patients and the renal artery deviated by less than 5 mm in four patients (mean deviation 2.7 mm) (Figure 2). If the deviations occur, manual adjustment is needed. Arteriography using diluted contrast material was performed only twice for initial aortography and final evaluation. Additional contrast injection during catheterization, guide wire manipulation, and positioning of a balloon catheter could be omitted by use of a roadmap. In all cases, PTRA was successful without complications and completed with a mean volume of contrast media of 18.1 ± 5.0 ml. No patients developed contrast-induced nephropathy. The mean volume of contrast media in PTRA with the overlay system was significantly decreased compared to that prior to the overlay (18.1 vs. 68.5 ml, p<0.01) (Figure 3). The procedure and fluoroscopic times were also significantly decreased (120.2 vs. 130.5 min, p<0.05, and 26.3 vs. 33.3 min, p<0.05, respectively) (Figure 3).Discussion
Herein, we demonstrated the usefulness of non-contrast MRA for a 3D-roadmap during PTRA. The 3D-roadmap showed sufficient visualization such that the overlaid vasculature on the live fluoroscopic image and several angiographic procedures could be omitted, resulting in a reduction of contrast media volume and fluoroscopic time. This novel technique is an effective method for performing PTRA in patients with chronic kidney disease who are limited in the use of contrast material. The most common reasons for disagreement between the overlaid non-contrast MRA image and aortography were differences in patient body posture and/or in the respiratory phase between MRA and aortography. In addition, the suppression of bone intensity on MRA makes it difficult to accurately generate the bone volume compared with CT. Further adjustment of sequence and registration is needed for a more accurate overlay system.Conclusion
The overlay system using non-contrast MRA enables the completion of PTRA safely with fewer angiographic procedures, thus requiring lower volumes of iodinated contrast materials.Acknowledgements
No acknowledgement found.References
1. Glockner JF, Takahashi N, Kawashima A, et al. Non-contrast renal artery MRA using an inflow inversion recovery steady state free precession technique (Inhance): comparison with 3D contrast-enhanced MRA. J Magn Reson Imaging. 2010;31(6):1411–1418.
2. Utsunomiya D, Miyazaki M, Nomitsu Y, et al. Clinical role of non-contrast magnetic resonance angiography for evaluation of renal artery stenosis. Circ J. 2008;72(10):1627–1630.
3. Fukuda T, Matsuda H, Doi S, et al. Evaluation of automated 2D-3D image overlay system utilizing subtraction of bone marrow image for EVAR: feasibility study. Eur J Vasc Endovasc Surg. 2013;46(1):75–81.
Figures