3124
Quantitative T1 and T2* carotid atherosclerotic plaque imaging using 3D multi-echo phase-sensitive inversion recovery sequence: a feasibility study1Department of Medical Imaging, Faculty of Life Sciences, Kumamoto University, Kumamoto, Japan, 2Radiological Center, National Hospital Organization Kumamoto Saisyunsou Hospital, Kumamoto, Japan, 3Graduate School of Health Sciences, Kumamoto University, Kumamoto, Japan, 4Radiological Center, National Hospital Organization Kumamoto Medical Center, Kumamoto, Japan
Synopsis
A quantitative evaluation of plaques is required in MR plaque imaging. The purpose of this study was to determine whether the 3D multi-echo Phase-Sensitive Inversion Recovery sequence can improve the T1 intra-plaque hemorrhage (IPH)-to-muscle contrast while simultaneously providing accurate T1 and T2* values for an IPH. This sequence may have potential to improve plaque MR imaging and make it possible to obtain detailed information about the components of carotid atherosclerotic plaques.
PURPOSE
MR plaque imaging has been widely used to detect carotid atherosclerotic plaques and to clinically evaluate the vulnerability of plaques that consist of lipid cores or intra-plaque hemorrhage (IPH). It is well known that an IPH shows high signal intensity on a T1-weighted image. However, the IPH-to-muscle contrasts will change depending on the settings of the imaging parameters or pulse sequence.1 Therefore, a quantitative evaluation of plaques is required. Furthermore, Zhu et al. recently reported that the T2* value of plaque can characterize the type of hemorrhage and may be used to determine a risk factor for the rupture of a plaque.2 In this study, we applied a three-dimensional (3D) multi-echo phase-sensitive inversion recovery (mPSIR) sequence to plaque imaging because this sequence is expected to improve IPH-to-muscle contrasts.3 Moreover, this sequence can simultaneously provide T1 and T2* values of the plaque without any additional scans. The purpose of this study was to determine whether the mPSIR can improve the T1 IPH-to-muscle contrast while simultaneously providing accurate T1 and T2* values for an IPH.METHODS
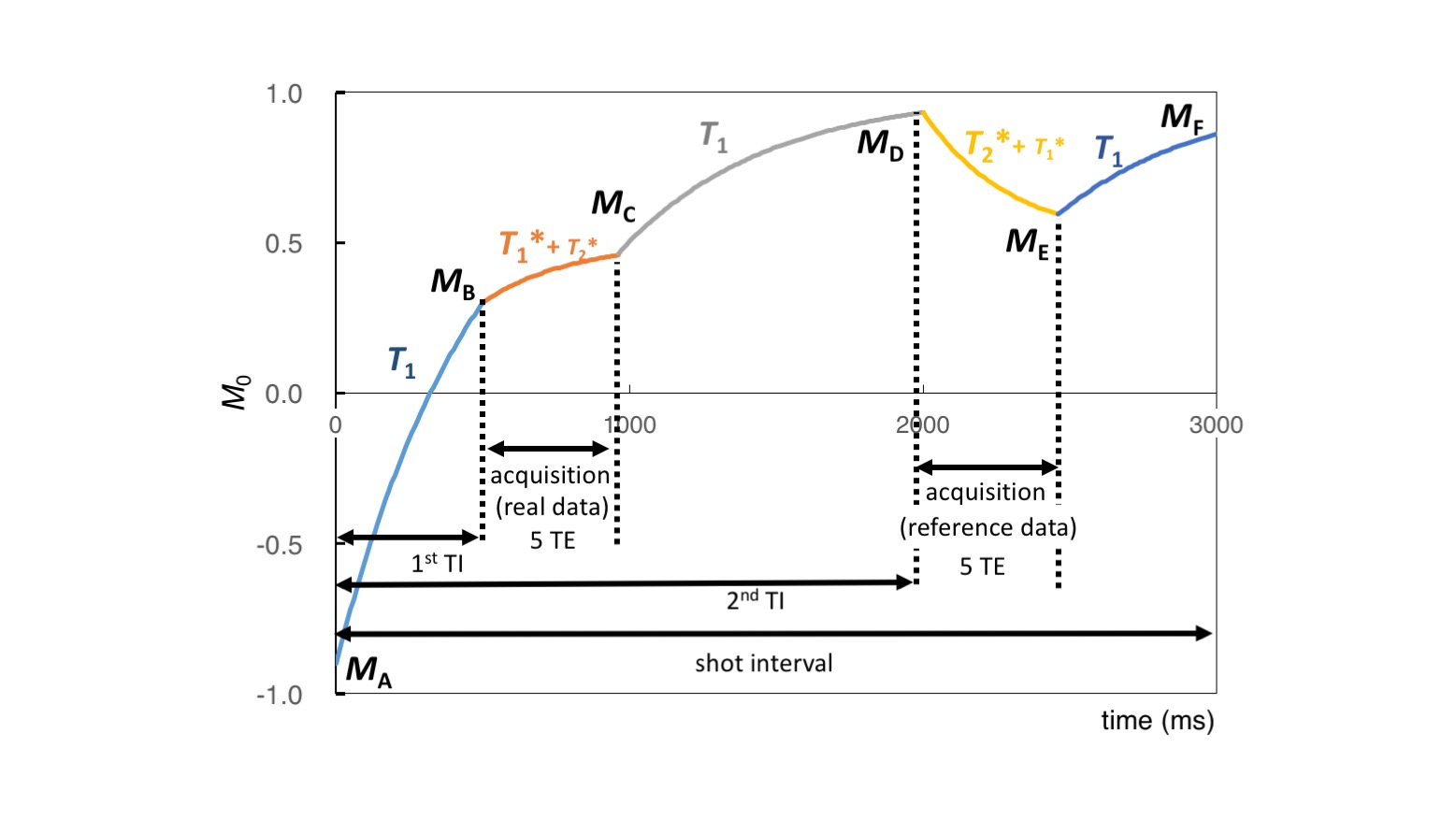
Each examination was performed using a 3.0 T MRI with a head-neck coil (Ingenia, Philips Healthcare). The study protocol was approved by the Institutional Review Board of our hospital. The mPSIR was performed using an inversion recovery turbo-field echo (IR-TFE) readout and centric k-space reordering. Figure 1 shows the magnetization evolution during the acquisition. For simultaneous T1 and T2* calculation, using two inversion times (TI) and multi-echo images (TE = 2.2, 4.5, 6.7, 8.9, 11.2 ms), we used two TI images acquired from IR prepared image data and reference data for which FA = 10°. Using the relationships between the two IR magnetization evolutions, the fully relaxed magnetization and T1 value were estimated in accordance with the iterative process reported by Warntjes MJB et al. .4 Moreover, using reference data in each of the TE images, the T2* values were estimated using non-linear least square fitting. To validate the T1 value, thirteen phantom tubes containing a mixture of 1.0 % agarose solution and different concentrations of Gd contrast agents were employed. The phantom were imaged using the mPSIR. The T1 values were calculated using the relationship between the two IR magnetizations in mPSIR with the first TE obtained in each acquisition. These phantoms were also imaged using a Look-Locker (L-L) and the T1 value was calculated for comparison with the mPSIR. Subsequently, to validate the T2* value, eight phantom tubes containing a mixture of 1.0 % agarose solution and different concentrations of superparamagnetic iron oxide (SPIO) contrast agents were used. The T2* values were calculated by non-linear least square fitting using five TE images obtained by reference acquisition for mPSIR. These phantoms were also imaged using a conventional turbo-field echo with multi-echo (mTFE) and the T2* values were calculated for comparison with the mPSIR. Ten healthy volunteers were enrolled in this study. All volunteer and an IPH-mimicking phantom with a T1 value of 392 ms images were obtained using the mPSIR, a conventional double IR turbo-spin echo (DIR-TSE), L-L and mTFE. The IPH phantom-to-muscle contrast of mPSIR was calculated and compared with that of DIR-TSE. To validate the simultaneous T1 and T2* values calculated using mPSIR, the T1 values of muscles were compared with those obtained using the L-L. The T2* values of vessel walls and muscles were compared to those obtained with the mTFE.RESULTS
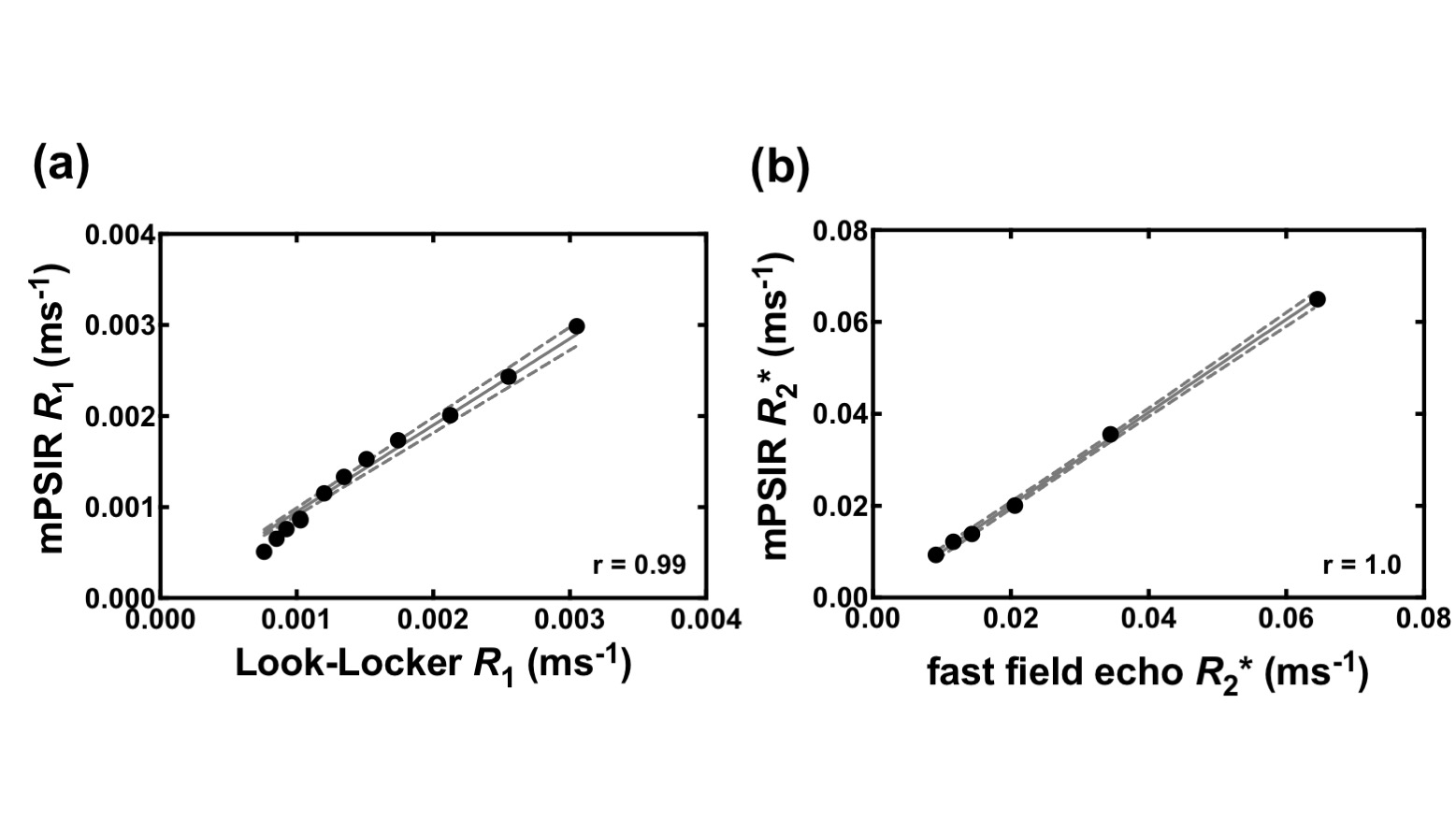
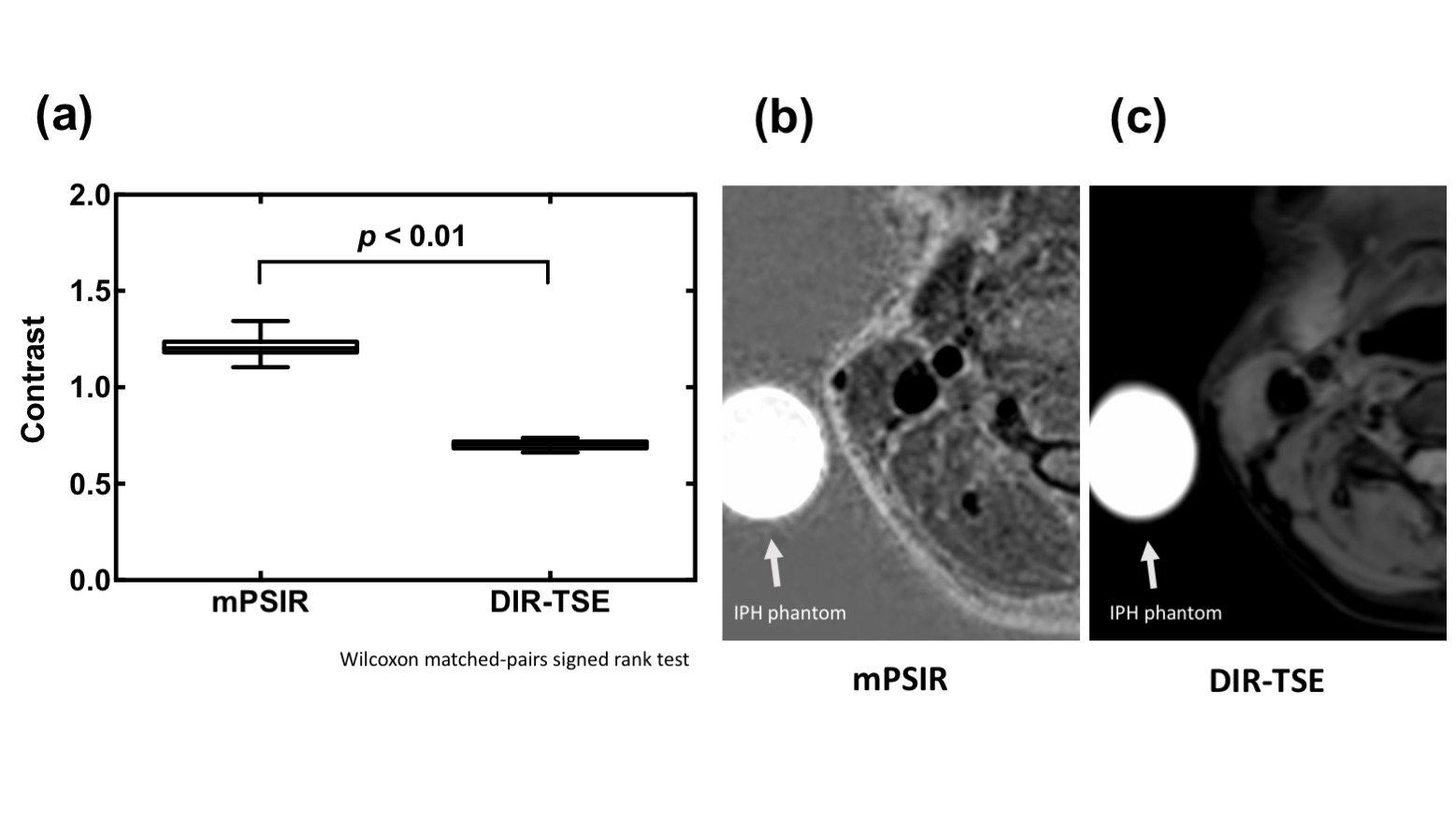
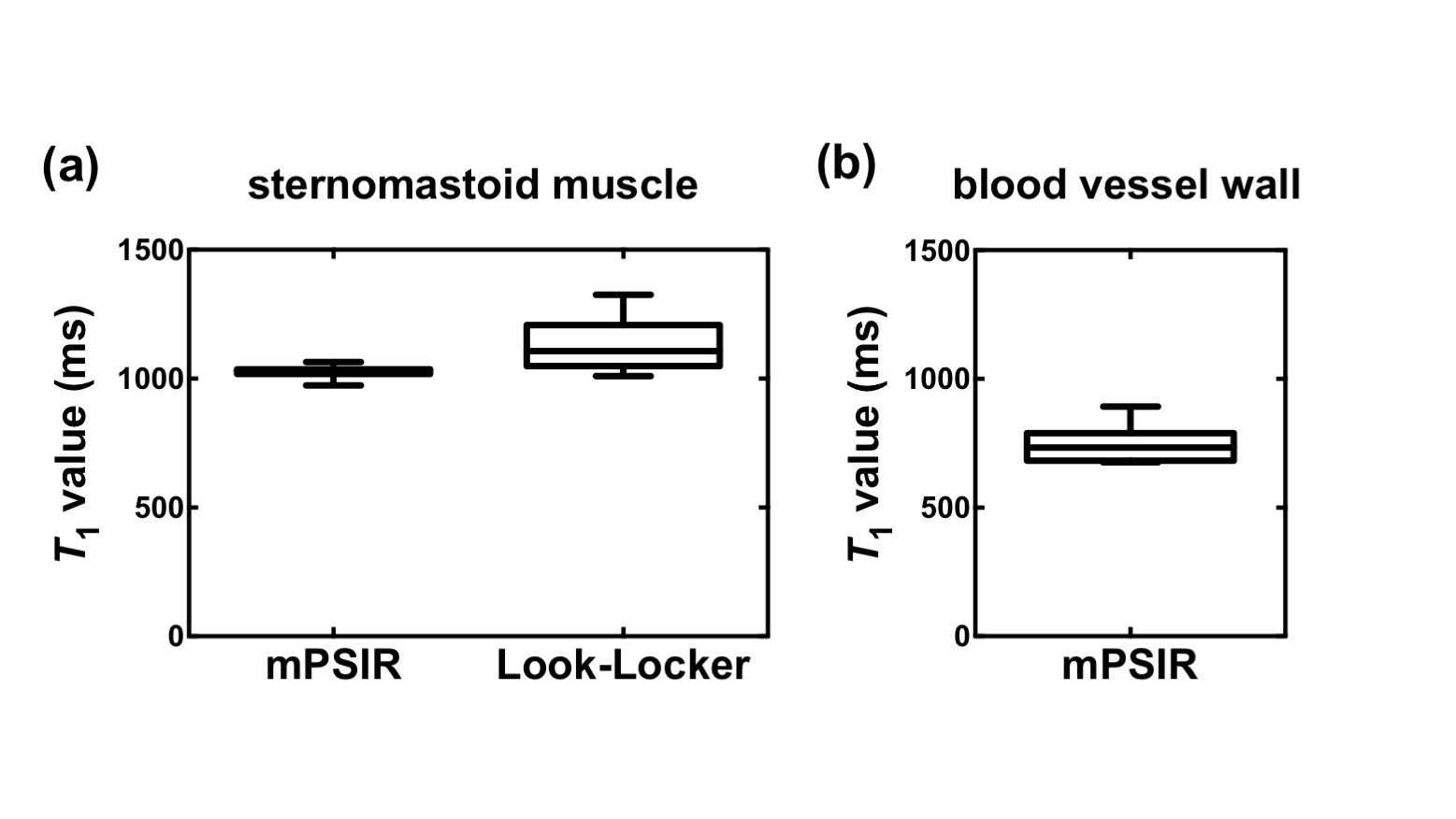
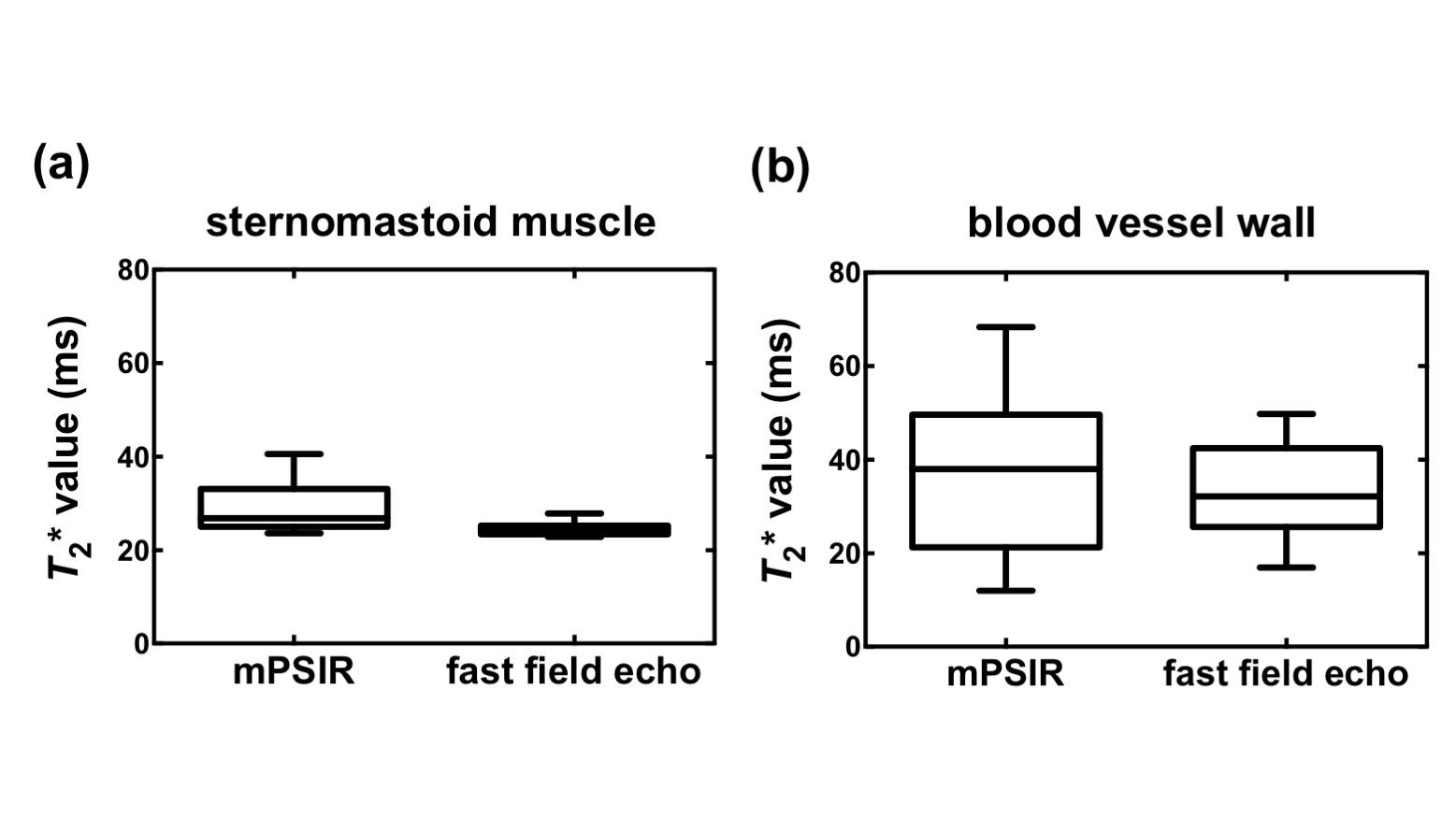
The estimated R1 (= 1/T1) values of Gd-containing phantom, measured using two TI images with first TE for mPSIR, were linearly correlated with those measured using L-L (Fig. 2a). The estimated R2* (= 1/T2*) values of the SPIO-containing phantom, measured using reference images for mPSIR, were also correlated with those measured by mTFE (Fig. 2b). In the in vivo study, the mPSIR demonstrated significantly higher IPH phantom-to-muscle contrasts than those of the DIR-TSE (Fig. 3). The estimated T1 values of the vessel walls and muscles in each subject, measured using mPSIR, were clearly correlated with those measured by L-L (Fig. 4). Moreover, the estimated T2* values of the vessel walls and muscles in each subject, measured using mPSIR, were clearly correlated with those measured using the mFFE sequence (Fig.5).DISCUSSION AND CONCLUSION
The mPSIR improved the T1 contrast between the IPH and peripheral tissue, while simultaneously providing accurate T1 and T2* values for the plaque region. Although further study is required to evaluate its clinical utility, this sequence may have potential to improve plaque MR imaging and make it possible to obtain detailed information about the components of carotid atherosclerotic plaques.Acknowledgements
No acknowledgement found.References
1. Saito A, Sasaki M, Ogasawara K, et al. Carotid plaque signal differences among four kinds of T1-weighted magnetic resonance imaging techniques: A histopathological correlation study. Neuroradiology 2012;54:1187–1194.
2. Zhu DC, Vu AT, Ota H, et al. An optimized 3D spoiled gradient recalled echo pulse sequence for hemorrhage assessment using inversion recovery and multiple echoes (3D SHINE) for carotid plaque imaging. Magn. Reson. Med. 2010;64:1341–1351.
3. Wang J, Börnert P, Zhao H, et al. Simultaneous noncontrast angiography and intraplaque hemorrhage (SNAP) imaging for carotid atherosclerotic disease evaluation. Magn. Reson. Med. 2013;69:337–345.
4. Warntjes MJB, Kihlberg J, Engvall J. Rapid T1 quantification based on 3D phase sensitive inversion recovery. BMC Med Imaging 2010;10:19.
Figures