3123
Aortic Vessel Wall Imaging Using 3D Phase Sensitive Inversion Recovery in Children and Young Adults1Pediatrics, Radiology, BME, University of Texas Southwestern Medical Center, Dallas, TX, United States, 2Pediatric Cardiology, Children's Medical Center Dallas, Dallas, TX, United States, 3Pediatrics, University of Texas Southwestern Medical Center, Dallas, TX, United States, 4Biomedical Engineering, King’s College, London, London, United Kingdom
Synopsis
Currently, T2-weighted TSE black blood zoom imaging (T2Z) is used to visualize atherosclerosis, but volumetric, high isotropic resolution datasets would be preferable. We compared aortic luminal sharpness (ALS) of a novel 3D bSSFP phase-sensitive inversion recovery black blood sequence (3DPSIR) to T2Z in 10 children and young adults with familial hypercholesterolemia at 5 aortic locations. 3DPSIR sequence duration was 7.0 minutes compared to 11.4 minutes for T2Z with no significant difference in ALS overall. 3DPSIR high resolution volumetric datasets will enable rapid, detailed 3D vessel wall imaging in children and young adults, allowing improved exploration of vascular health.
Introduction
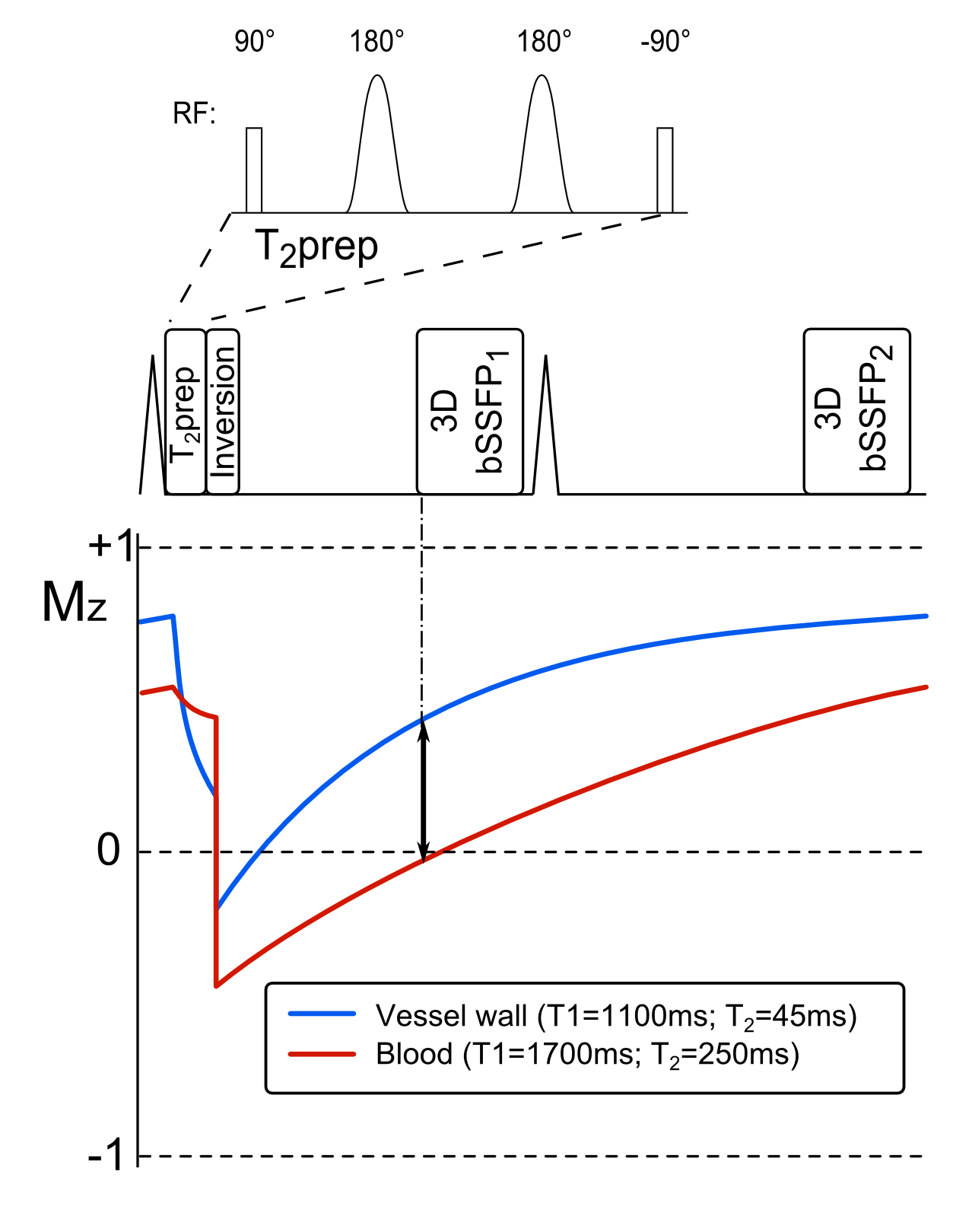
Two-dimensional (2D) EKG-triggered, turbo spin echo (TSE) black blood sequences can be used to image subclinical aortic atherosclerosis.1 The value of this sequence for cardiovascular risk stratification has been demonstrated in more than 2500 patients as part of the Framingham Heart Study2,3 and in populations such as familial hypercholesterolemia.4 Currently, T2-weighted, free-breathing, EKG-triggered, TSE black blood zoom imaging (T2Z) allows complete coverage of the thoracic aorta in a timely fashion.5 However, due to the tortuous nature of the aorta, it would be preferable to obtain volumetric datasets with high isotropic resolution to improve visualization of aortic atherosclerosis. This would also avoid slice mis-registration which commonly hampers 2D techniques. We aimed to compare the T2Z method to a novel 3D, balanced steady state free precession (bSSFP), respiratory navigated, phase-sensitive inversion recovery black blood imaging sequence (3D PSIR, Figure 1) in children and young adults to potentially improve vessel wall imaging in this population.Methods
Children and young adults with familial hypercholesterolemia were recruited as part of a study on vascular health. The study was IRB approved at UT Southwestern. Volunteers underwent a cardiac MRI (CMR) study including the T2Z and 3D PSIR sequences on a Philips 1.5T Ingenia scanner, without sedation or breath-holding. The imaging plane was in a para-sagittal plane to cover the aorta from the top of the arch to the level of the diaphragm. T2Z imaging parameters were: voxel size=1.0 x 1.2 x 5 mm3; FOV 260 x 55 mm; TR=2 cardiac cycles, TE=50 ms; echo train length=10; 2 signal averages. 3D PSIR imaging parameters were: voxel size=0.8 x 0.8 x 1.6 mm3; FOV 300 x 300 x 68 mm; flip angle 70°; TR=3.48 ms; TE=1.74 ms; TI=400 ms; echo train length=45; respiratory navigation with 5 mm gating window. Trigger delay was set as longest for both sequences.
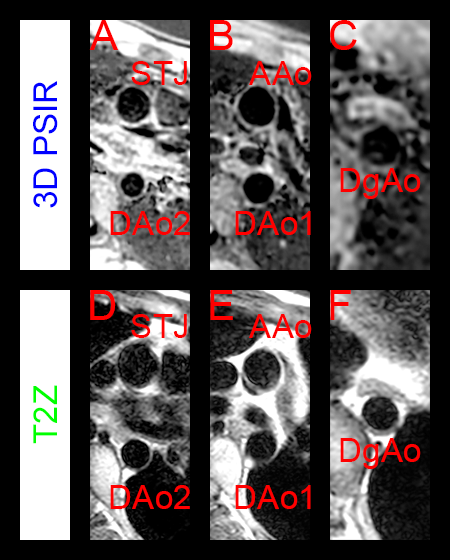
For analysis, three axial slices of the 3D PSIR were chosen at the aortic sinotubular junction (STJ), the ascending aorta just above the right pulmonary artery (AAo), and the aorta at the diaphragm (DgAo); the descending aorta at the level of the AAo and STJ were also analyzed (DAo1 and DAo2, respectively). Figure 2 shows example 3D PSIR (panels A-C) and T2Z (D-F) images at the STJ and DAo2 level (A, D), AAo and DAo1 level (B, E), and DgAo level (C, F). Using a 3D image linking tool, the closest T2Z image was chosen for comparative analysis. Aortic luminal sharpness was measured using SoapBubble 5.0 (Philips Medical Systems, Amsterdam, The Netherlands). Paired luminal sharpness and duration data were tested using Wilcoxon signed-rank test. Statistical analysis was performed using GraphPad Prism 7.0.
Results
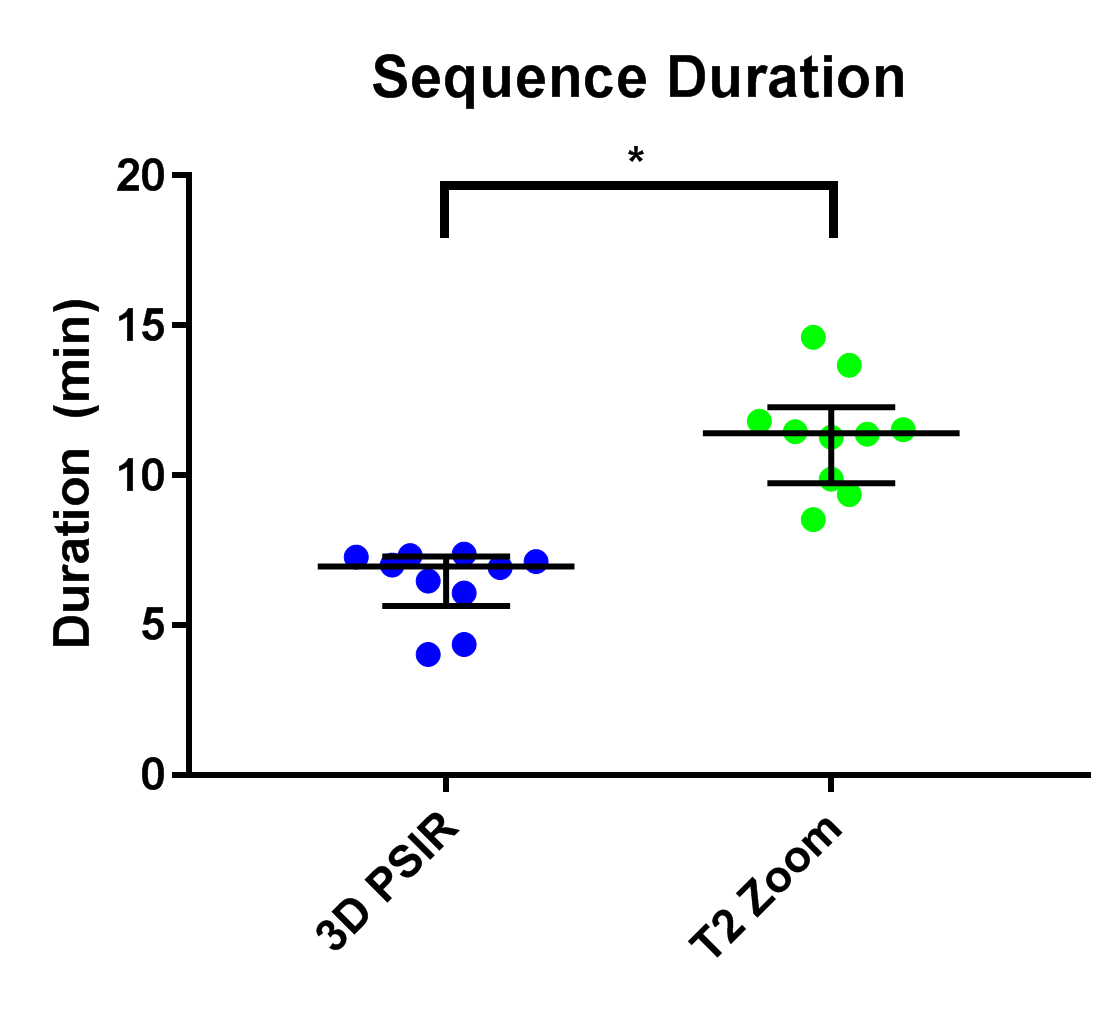
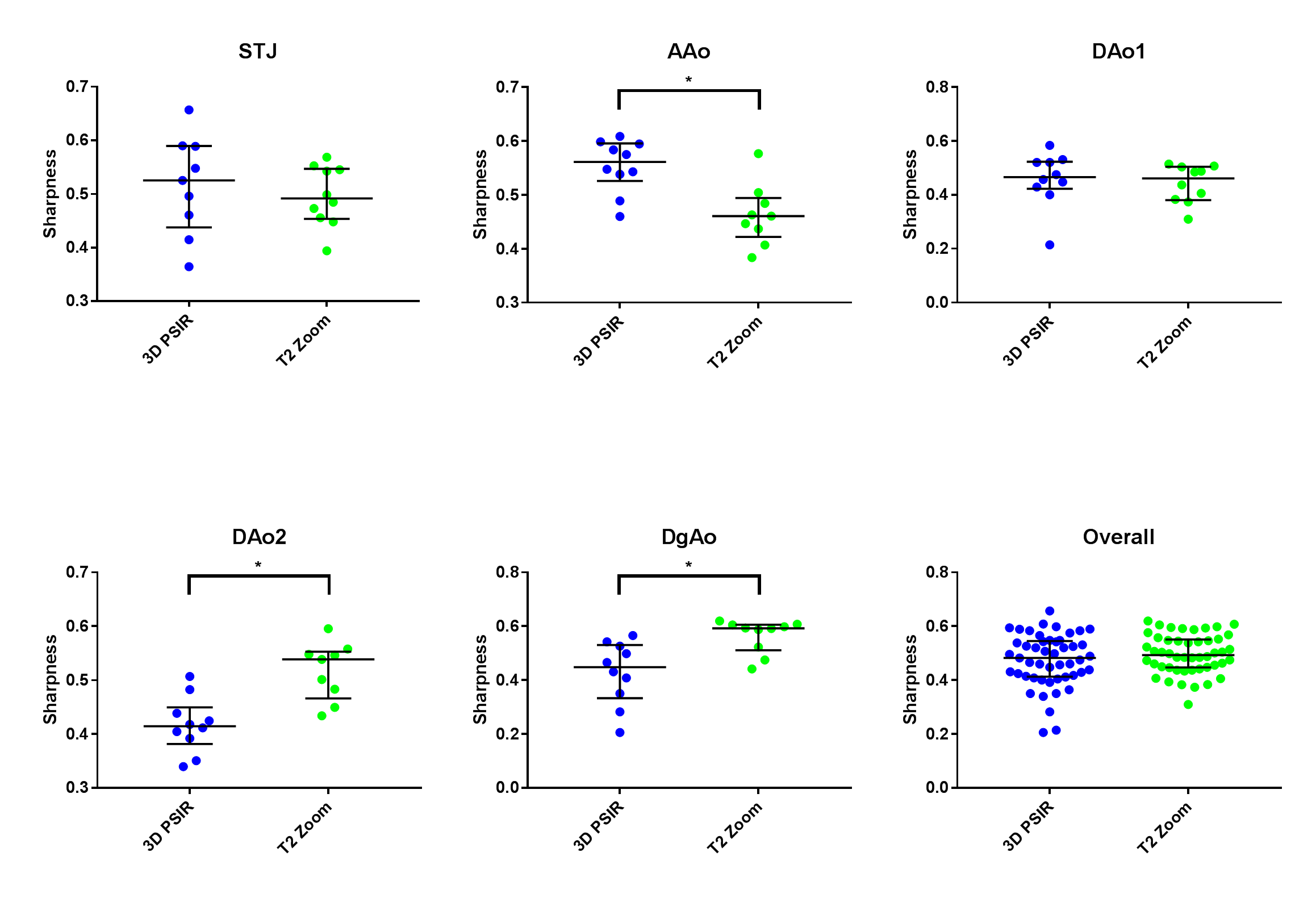
Ten patients (median age 15.2 years, range 7.3-19.5) underwent the above protocol. Three vessel tracings (one 3D PSIR of the STJ, one T2Z of the AAo, and one T2Z of the DAo2) were unable to be analyzed. The median duration of the 3D PSIR sequence was 7.0 minutes (interquartile range 6.2-7.2), compared to 11.4 (10.2, 11.7) minutes for the T2Z sequence (39% reduction), and was always faster (Figure 3). Luminal sharpness was better on the 3D PSIR at the AAo, and better on T2Z at the DAo2 and DgAo; overall, there was no significant difference in aortic luminal sharpness between 3D PSIR and T2Z (Figure 4).Discussion
The 3D PSIR sequence allows volumetric depiction of the aorta with high isotropic resolution and has equivalent luminal sharpness to the standard T2Z sequence with shorter sequence duration. The advantage of reduced slice thickness in the isotropic dataset may avoid the loss of information that occurs from partial volume effects, and therefore allow for improved atheroma detection and thus more accurate risk stratification. However, the atheroma burden in this group of young patients receiving statin therapy was low, and therefore we were unable to evaluate the difference in sensitivity for atheroma quantification between the two sequences.Conclusion
The development of the 3D PSIR sequence will enable a rapid and more detailed 3D vessel wall dataset, allowing improved exploration of vascular health in children and young adults. This may yield further insights into patient risk stratification for diseases that cause vascular changes in children such as familial hypercholesterolemia, as well as obesity and hypertension.Acknowledgements
No acknowledgement found.References
1. Fayad ZA, Fallon JT, Shinnar M, et al. Noninvasive in vivo high-resolution magnetic resonance imaging of atherosclerotic lesions in genetically engineered mice. Circulation. 1998;98(15):1541-7.
2. Jaffer FA, O'Donnell CJ, Larson MG, et al. Age and sex distribution of subclinical aortic atherosclerosis: a magnetic resonance imaging examination of the Framingham Heart Study. Arterioscler Thromb Vasc Biol. 2002;22(5):849-54.
3. Oyama N, Gona P, Salton CJ, et al. Differential impact of age, sex, and hypertension on aortic atherosclerosis: the Framingham Heart Study. Arterioscler Thromb Vasc Biol. 2008;28(1):155-9.
4. Schmitz SA, O'Regan DP, Fitzpatrick J, et al. Quantitative 3T MR imaging of the descending thoracic aorta: patients with familial hypercholesterolemia have an increased aortic plaque burden despite long-term lipid-lowering therapy. J Vasc Interv Radiol. 2008;19(10):1403-8.
5. Hussain T, Clough RE, Cecelja M, et al. Zoom imaging for rapid aortic vessel wall imaging and cardiovascular risk assessment. J Magn Reson Imaging. 2011;34(2):279-85.
Figures