3112
Dependence of the Precision of Myocardial Late Gadolinium Enhancement Quantification on Inversion Time Selection Simulated Using Synthetic Inversion Recovery MR Imaging1Department of Radiology and Radiological Science, Medical University of South Carolina, Charleston, SC, United States, 2Leiden University Medical Center, Leiden, Netherlands
Synopsis
Clinical late gadolinium enhancement (LGE) imaging of the myocardium requires inversion time (TI) optimization for adequate image quality. As the optimal TI (TI0) depends on various factors, its influence on the precision of myocardial LGE quantification is of interest. In this study we aimed to prospectively investigate how the precision of LGE quantification varies in the clinically relevant TI range in 53 patients using T1-mapping-based synthetic inversion recovery (IRsynth) approach. We concluded that phase-sensitive IRsynth images provide precise quantification independent of TI, while magnitude IRsynth-based quantification is precise at TI0 or longer TIs, but showing decreased precision below TI0.
Purpose
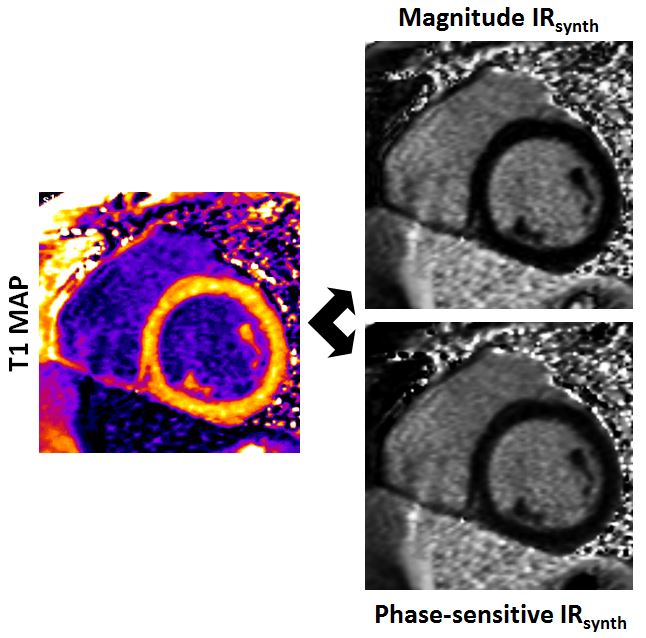
Magnitude-reconstructed inversion recovery (IR) late gadolinium enhancement (LGE) acquisition requires inversion time (TI) adjustment in order to achieve distinguishable signal difference between normal and enhanced myocardium. The optimal TI value (TI0) depends on various factors1, and typically increases in the time post-contrast. Since T1-mapping-based synthetic IR (IRsynth) images can be generated at any theoretical TI (Figure 1)2, these images are suitable to retrospectively evaluate the TI0 setting or range at any post-contrast time point. Accordingly, the purpose of our study was to investigate the influence of TI on the precision of myocardial LGE quantification in IRsynth images in comparison with conventional techniques in patients with ischemic LGE to define an optimal TI range in which LGE evaluation can be precisely performed.Methods
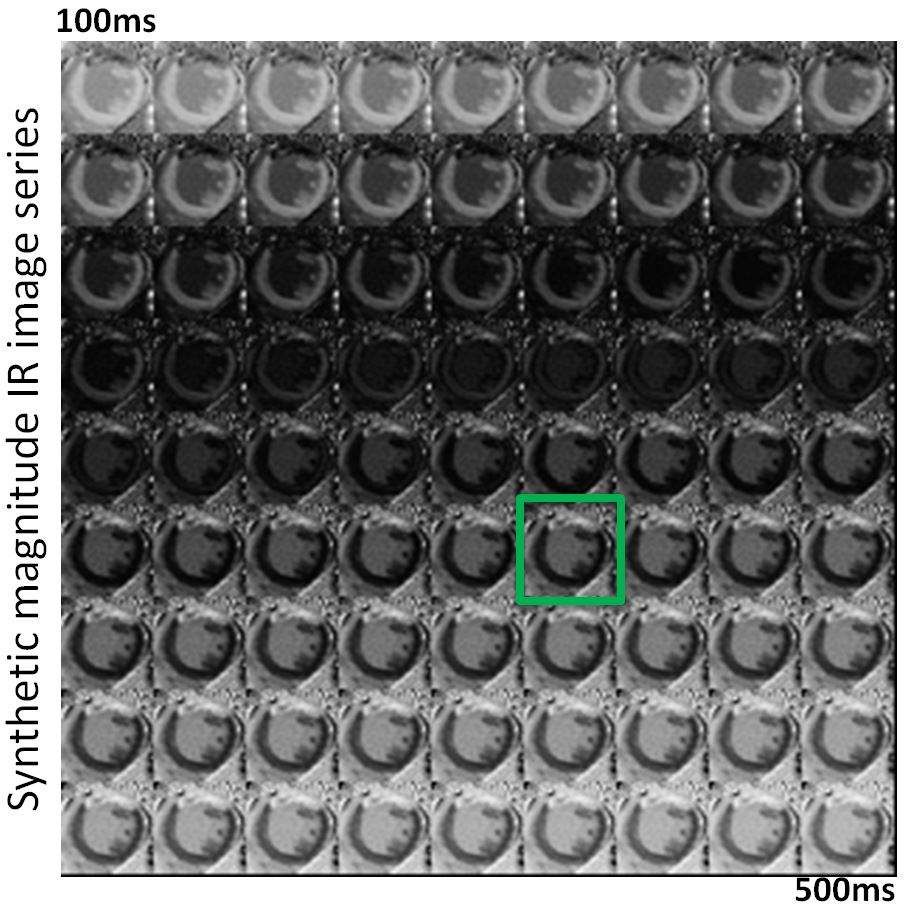
From June 2014 to June 2015, 53 consecutive patients referred for viability cardiac MRI were prospectively enrolled in this IRB approved study. Patients underwent cardiovascular MRI on a 1.5T system (MAGNETOM Avanto, Siemens Healthcare, Erlangen, Germany). Twelve minutes post-contrast (0.1mmol/kg gadobenate-dimeglumine), short-axis IR images were generated using a steady-state free-precession (SSFP) based IR sequence (Field-of-view 340×255mm2; section thickness 8mm; acquisition matrix 192×106; in-plane resolution 1.77×1.77mm2; TE/TR 1.1/2.6ms; bandwidth 965Hz/pixel; and flip angle 50°). Images were reconstructed in both magnitude and phase-sensitive fashion. T1-mapping was performed immediately after conventional LGE imaging using an investigational prototype MOLLI sequence (Scheme of 4(1)3(1)2; other parameters matched, except: TE/TR 1.1/2.6ms; bandwidth 1085Hz/pixel; and flip angle 35°). A set of 81 IRsynth images with 5ms TI increments were generated as previously described (Figure 2).2 Myocardial LGE was measured using a threshold-based algorithm (5SD)3, and differences in the area of LGE measured at various TIs were compared using a one-way analysis of variance.Results
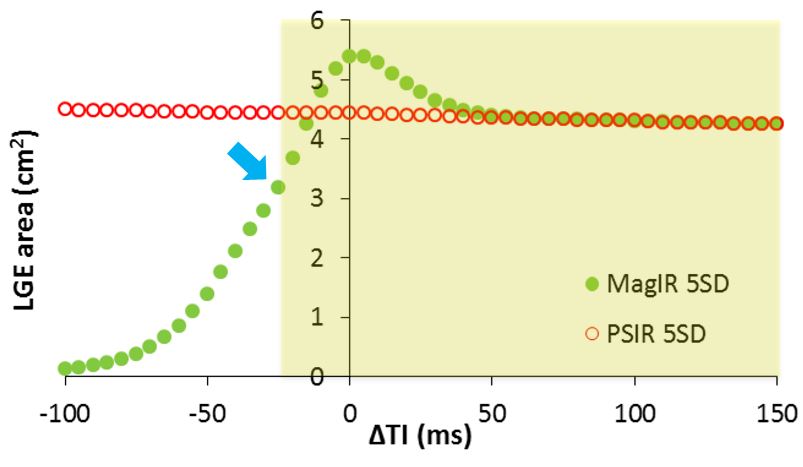
IRsynth images were successfully generated for every patient. Twenty patients showed ischemic myocardial LGE. The average TI used for conventional LGE acquisition was 321±17ms, while TI0 in the IRsynth image set was 311±29ms (P=0.067). The conventional and IRsynth techniques yielded similar areas of infarct at TI0 (magnitude 5.68±1.61 vs. 5.21±1.43cm2 (P=2024); phase-sensitive 4.92±1.66 vs. 4.38±1.47cm2 (P=0.1136). The TI dependence of the precision of LGE area measurements by the magnitude and phase-sensitive IRsynth methods is shown in Figure 3. The magnitude IRsynth technique provided precise assessment of LGE area at TIs greater than or equal to TI0, while precision was decreased below TI0. The quantified LGE area showed significant differences at 25ms below TI0 (P<0.001). LGE area measurements did not show any significant difference over the analyzed TI range in the phase-sensitive IRsynth image sets.Discussion
In this study, we investigated the influence of TI on the precision of LGE area quantification using IRsynth approaches. Our results indicate that LGE quantification using phase-sensitive IRsynth images provides consistent LGE area assessment over a wide, clinically relevant TI range, while magnitude IRsynth images show decreased precision below a certain TI level. Our results also suggest that prospective TI optimization using a Look-Locker TI-scout sequence may not be necessary before LGE imaging, as any TI within 150ms above TI0 provides good precision. However, this conclusion may not be fully applicable to conventional LGE techniques. While the clinical relevance of these results may be limited at sites where phase-sensitive IR imaging is available, the IRsynth approach may provide substantial benefits for research where quantification of LGE size is important. This is especially true in multicenter trials in which the experience levels of the observers vary and where IRsynth imaging may help standardize image evaluation by eliminating confounding operator-dependent factors from image acquisition and analysis.Conclusions
In conclusion, the results of our study indicate that the precision of LGE area quantification using magnitude IRsynth images is reliable over a wide TI range but only at or above TI0, while the precision using phase-sensitive IRsynth images is consistent over the entire clinically relevant TI range. Synthetic T1-based IR images are reliable for LGE quantification and may provide benefit over conventional LGE methods by eliminating the effects of operator dependence.Acknowledgements
No acknowledgement found.References
1. Simonetti OP, Kim RJ, Fieno DS, et al. An improved MR imaging technique for the visualization of myocardial infarction. Radiology 2001;218(1):215-223.
2. Varga-Szemes A, van der Geest RJ, Spottiswoode BS, et al. Myocardial Late Gadolinium Enhancement: Accuracy of T1 Mapping-based Synthetic Inversion-Recovery Imaging. Radiology 2016;278(2):374-382.
3. Amado LC, Gerber BL, Gupta SN, et al. Accurate and objective infarct sizing by contrast-enhanced magnetic resonance imaging in a canine myocardial infarction model. J Am Coll Cardiol 2004;44(12):2383-2389.
Figures