3096
Ultrafast Cardiac Balanced Inversion Recovery with Interleaved Acquisition (UF-CABIRIA) for improved simultaneous T1 and T2 quantification of the heart at 3T.1Division of Radiological Physics, University of Basel Hospital, Basel, Switzerland, 2Department of Biomedical Engineering, University of Basel, Basel, Switzerland
Synopsis
CABIRIA is a method for the simultaneous quantification of T1 and T2 values of the myocardium. As other T1-quantification sequences, it relies on a bSSFP readout, and it is thus susceptible to off-resonance effects. In this work, we show an improvement over the CABIRIA method that reduces the TR and therefore increases the robustness towards field inhomogeneities. This method can potentially be extended to other quantification techniques.
Introduction
Cardiac relaxometry has attracted considerable interest in the last years for diagnosis of both diffuse and focal pathologies of the myocardium. Recently, a method for simultaneous quantification of T1 and T2, named Cardiac Balanced Inversion Recovery with Interleaved Acquisition (CABIRIA) was proposed1. CABIRIA is based on an inversion pulse followed by a balanced steady state free precession (bSSFP) readout, also common to a number of other cardiac T1 quantification methods2-4. Generally, all bSSFP-based methods are off-resonance sensitive to some extent5,6, leading to quantification inaccuracies. In this work, the repetition time (TR) of the CABIRIA sequence is shortened using a recently proposed SSFP optimization strategy for lung imaging7 to reduce its sensitivity to field inhomogeneities.Methods
The CABIRIA method is based on an adiabatic inversion pulse followed by a continuous train of single-shot Cartesian bSSFP kernels encoding the recovery curve. After a free recovery period, the acquisition is repeated with a delay between the inversion and acquisition realized with dummy TRs1. In this work, the bSSFP kernels of CABIRIA were optimized by reducing the excitation duration and improving the gradient switching patterns by using overlapping ramps and asymmetric readout, in a similar way as described in7,8. This optimized version, termed ultrafast-CABIRIA (uf-CABIRIA) was compared to a conventional CABIRIA implementation in a phantom and in vivo. The phantom experiment was performed with a spherical homogeneous phantom, and the shim was tweaked in order to obtain a linearly increasing frequency shift across the phantom. The acquisition parameters for uf-CABIRIA were: resolution 1.33x1.33x8mm3, matrix size 256x208, bandwidth 1775Hz/px, flip angle 35°, total acquired images 50. The achieved TR/TE for the uf-CABIRIA sequence was 2.1/0.7ms. The CABIRIA sequence was resolution-matched and had a bandwidth if 1550Hz/px and a TR/TE of 2.9/1.3ms. For the in vivo experiment, the same acquisition parameters were used and an additional CABIRIA acquisition with a lower resolution, and therefore lower TR, was also acquired for comparison. The parameters of the low-resolution CABIRIA were resolution 1.7x1.7x8mm3, matrix size 192x162, bandwidth 1530Hz/px, TR/TE 2.7/1.19ms. A single slice of a mid-ventricular short axis view of the heart was acquired in a healthy volunteer. T1 and T2 maps were calculated using the procedure described in1. In the phantom, a longitudinal profile of the acquired maps was extracted and compared between the two different methods. The in vivo images were visually compared and manual segmentation was performed according to the American Heart Association 17-segment model. The variation of the quantitative values across the segments was analyzed.Results
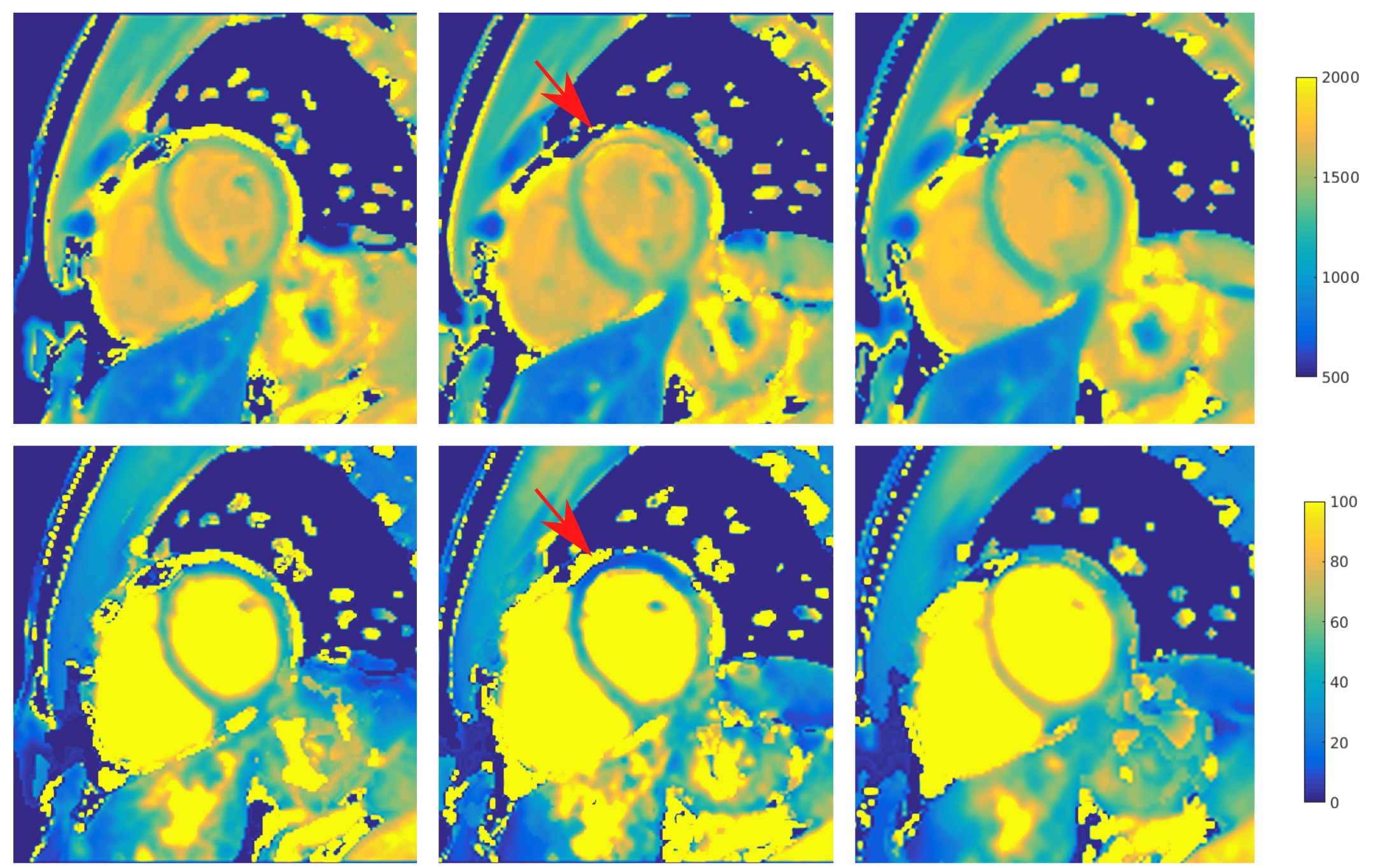
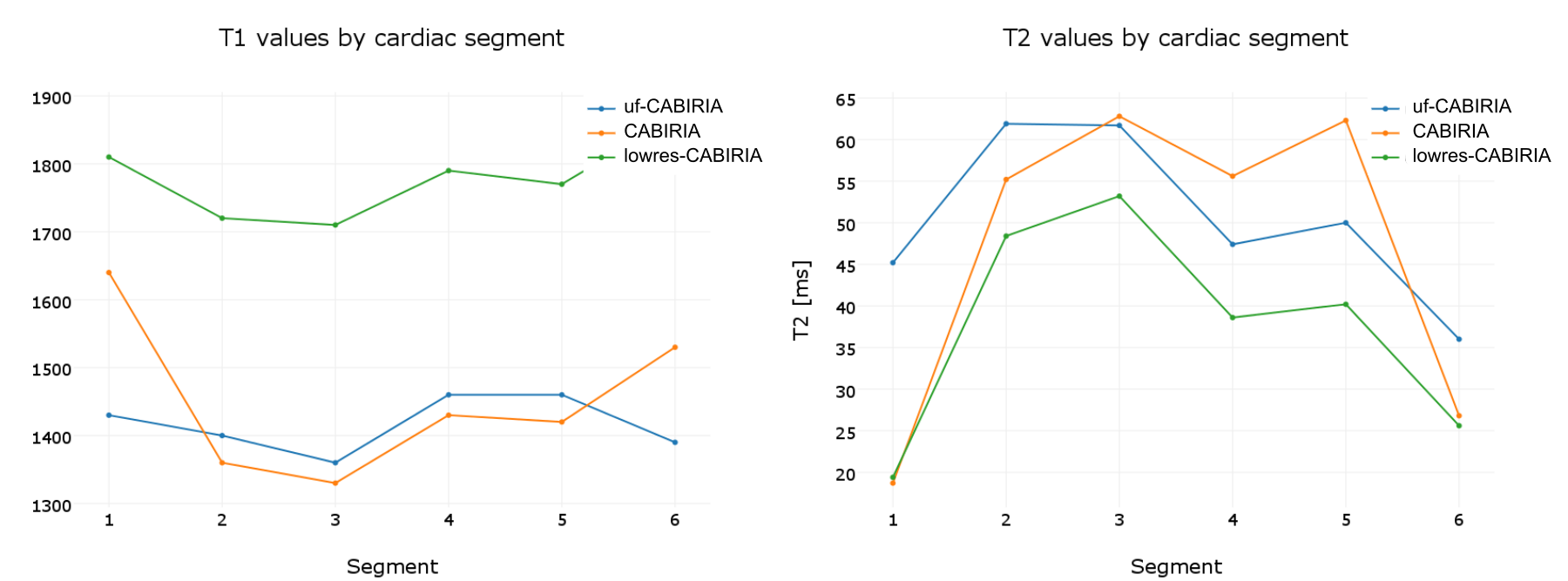
The uf-CABIRIA sequence allowed a TR reduction of 28%, consequentially leading to an increase of the bSSFP passband by 40%. The phantom experiments showed a clear difference in sensitivity between the two sequences, the uf-CABIRIA sequence having a larger area of homogeneity and especially a more consistent behavior in T2 quantification (fig. 1). In the in vivo acquisition, an off-resonance-related bias is apparent for the CABIRIA T1 and T2 maps in the anterior and anterolateral regions, being more pronounced in T2. The uf-CABIRIA shows the same but damped inhomogeneity pattern. Similar, from the shortened TR, the low resolution CABIRIA scan is less affected by inhomogeneities but suffers from significant partial volume effects (fig. 2). Segmentation confirms the visual inspection of decreased values in the anterior and anterolateral segments for CABIRIA that become less pronounced for uf-CABIRIA (fig. 3).Discussion
The optimizations introduced to the uf-CABIRIA acquisition markedly enhanced T1 and T2 mapping in cardiac regions affected by B0 inhomogeneity, namely for the anterior and anterolateral segments that are close to the airspace of the lungs. Decreasing the resolution in order to reduce the TR of a conventional CABIRIA acquisition similarly redices the off-resonance sensitivity, but at the cost of increased partial volume effects affecting precision. Overall, no artifacts from the TR acceleration were visible in the images, thus recommending uf-CABIRIA for cardiac imaging, especially at higher field strengths.Conclusion
CABIRIA, and possibly other bSSFP-based cardiac relaxometry sequences, such as MOLLI, can benefit from a shortening of the TR using a recently proposed optimization strategy for ufSSFP imaging to improve quantification robustness in the presence of B0 inhomogeneities.Acknowledgements
This work was partly supported by Siemens Healthineers.References
1. Santini F, Kawel-Boehm N, Greiser A, Bremerich J, Bieri O. Simultaneous T1 and T2 quantification of the myocardium using cardiac balanced-SSFP inversion recovery with interleaved sampling acquisition (CABIRIA). Magn. Reson. Med. 2015;74:365–371. doi: 10.1002/mrm.25402.
2. Messroghli DR, Radjenovic A, Kozerke S, Higgins DM, Sivananthan MU, Ridgway JP. Modified Look-Locker inversion recovery (MOLLI) for high-resolution T1 mapping of the heart. Magn. Reson. Med. Off. J. Soc. Magn. Reson. Med. Soc. Magn. Reson. Med. 2004;52:141–146. doi: 10.1002/mrm.20110.
3. Chow K, Flewitt JA, Green JD, Pagano JJ, Friedrich MG, Thompson RB. Saturation recovery single-shot acquisition (SASHA) for myocardial T(1) mapping. Magn. Reson. Med. 2014;71:2082–2095. doi: 10.1002/mrm.24878.
4. Piechnik SK, Ferreira VM, Dall’Armellina E, Cochlin LE, Greiser A, Neubauer S, Robson MD. Shortened Modified Look-Locker Inversion recovery (ShMOLLI) for clinical myocardial T1-mapping at 1.5 and 3 T within a 9 heartbeat breathhold. J. Cardiovasc. Magn. Reson. Off. J. Soc. Cardiovasc. Magn. Reson. 2010;12:69. doi: 10.1186/1532-429X-12-69.
5. Kellman P, Hansen MS. T1-mapping in the heart: accuracy and precision. J. Cardiovasc. Magn. Reson. 2014;16:2. doi: 10.1186/1532-429X-16-2.
6. Kellman P, Herzka DA, Arai AE, Hansen MS. Influence of Off-resonance in myocardial T1-mapping using SSFP based MOLLI method. J. Cardiovasc. Magn. Reson. 2013;15:63. doi: 10.1186/1532-429X-15-63.
7. Bieri O. Ultra-fast steady state free precession and its application to in vivo (1) H morphological and functional lung imaging at 1.5 tesla. Magn. Reson. Med. Off. J. Soc. Magn. Reson. Med. Soc. Magn. Reson. Med. 2013. doi: 10.1002/mrm.24858. 8. Bauman G, Santini F, Pusterla O, Bieri O. Pulmonary relaxometry with inversion recovery ultra-fast steady-state free precession at 1.5T. Magn. Reson. Med. 2016. doi: 10.1002/mrm.26490.
Figures