3091
Probing metabolic alterations in lung injury during protective and non-protective ventilation using hyperpolarized [1-13C] pyruvateMehrdad Pourfathi1, Yi Xin1, Maurizio Cereda2, Stephen Kadlecek1, Harrilla Profka1, Hooman Hamedani1, Ian Duncan1, Sarmad Siddiqui1, Nicholas Drachman1, Kai Ruppert1, and Rahim Rizi1
1Radiology, University of Pennsylvania, Philadelphia, PA, United States, 2Anesthesiology and Critical Care, University of Pennsylvania, Philadelphia, PA, United States
Synopsis
In this study, hyperpolarized [1-13C]-pyruvate imaging was used to investigate the effect of positive-end expiratory pressure (PEEP) on the stabilization of lung metabolism after injury. Results demonstrated significantly lower lactate-to-pyruvate ratio in rats ventilated with PEEP.
Introduction
Ventilator induced lung injury (VILI) results from mechanical trauma and secondary inflammatory responses. Protective ventilation and positive-end expiratory pressure (PEEP) can attenuate cytokine concentrations and inflammatory infiltrates due to atelectasis (atelectrauma), protecting the lungs from the progression of pre-existing lung inflammation [1,2]. Previous metabolic imaging studies have focused on how glucose uptake is affected by ventilator settings. In this study, the conversion of hyperpolarized [1-13C]-pyruvate to [1-13C]-lactate was used to investigate the effect of PEEP on the stabilization of lung metabolism after injury.Methods
Seven Sprague-Dawley rats (341±38g) were ventilated with a tidal volume (TV) of 8.1±0.8 mL/kg and PEEP of 7±2cmH2O (protective ventilation) for t=60min, followed by tracheal hydrochloric acid (pH 1.25, 1.0mL/kg) instillation at t=70min. These ventilation settings were maintained until t=120min. PEEP was then lowered to zero in four rats and kept stable until the end of the experiment (t=300min) in three rats. Dynamic pulmonary compliance was calculated in the absence of PEEP by dividing peak inspiratory pressure measured via pressure meter by the TV delivered to the rat, and was used to monitor injury progression [3]. Rats were imaged in supine position using a 1H/13C quadrature birdcage coil (m2m) at 4.7T (Varian Inc.). Proton images were acquired using a multi-slice gradient-echo sequence (TR/TE=80/1.5ms, α=10°, 128x128 voxels). Hyperpolarized [1-13C]-pyruvate imaging was conducted at t=60min (baseline), t=120min (follow-up 1), and t=300min (follow-up 2). ~22 µL of [1-13C]-pyruvate was polarized using a HyperSense DNP polarizer to over 25%. The sample was melted using 4mL of a dissolution buffer (40mM Trizma, 160mM NaOH, 50mM NaCl, 0.1g/L EDTA) at 180°C to yield a neutralized isotonic solution of 80mM [1-13C]-pyruvate at ~37°C. 12 seconds after dissolution, 4ml/kg of the hyperpolarized agent was administered via the tail-vein over 6s. A single-slice axial carbon-13 chemical shift image was acquired using a 16x16 FID-CSI sequence (TR/TE=35/0.35ms, α=12°), with a custom outward spiral k-space trajectory [4]. Imaging started 12 seconds after the end of injection (in-plane FOV=45x45mm2, 15mm slice thickness). A 12s breath-hold was applied to minimize the respiratory motion artifact during carbon imaging. Blood oxygen level was monitored using a pulse oximeter during the scan. The peaks in the phase-corrected real part of the spectra was fit to Lorentizan functions and metabolites were quantified by finding the area under the fits using custom-made routines in MATLAB2014b. Processed carbon images were converted to DICOM format and overlaid on the proton image using OsiriX 8.0.Results and Discussion
Figure 1 shows pyruvate and lactate maps overlaid on proton images before and four hours after instillation of HCl in a rat ventilated with no PEEP. The intensity of each image is normalized to its own maximum intensity. The images show increased pyruvate and lactate signal post-injury. The increased pyruvate signal was likely due to increased capillary permeability, while the enhanced lactate signal was chiefly caused by an inflammatory response to the acute injury characterized by neutrophilic infiltration in the lungs [5-6]. Figure 2 shows the average lactate-to-pyruvate (top) and pulmonary compliance (bottom) measured for each group at three different time points. Average lactate-to-pyruvate ratio increased by 16% in rats ventilated with PEEP between hours 2 and 5. However, this ratio increased by 76% in the rats ventilated with no PEEP (p<0.05). The observed effect size (Cohen’s d) for this measurement was 1.67. Rats ventilated without PEEP had a significant decline of compliance at the 5-hour time point compared with the rats ventilated with PEEP (p<0.01), indicating lung injury progression and atelectasis.Conclusions
This study used hyperpolarized [1-13C]-pyruvate imaging to investigate differences in metabolism of injured lungs after protective and non-protective ventilation. The significant increase observed in the lactate-to-pyruvate ratio is due to the recruitment of neutrophils caused by atelectrauma and by over-distention of the ventilated alveoli leading to VILI [5-6]. Increased progression of lung injury in rats ventilated with no PEEP is confirmed by the significant decline in pulmonary compliance at the 5-hour time point compared to rats ventilated with PEEP. This study shows that in the presence of pre-existing lung injury, hyperpolarized carbon-13 MRI can detect secondary inflammation in the absence of PEEP by measuring changes in cellularity and bioenergetics of the lungs. This information is critical for early detection and management of lung injury.Acknowledgements
This work was supported by the National of Institutes of Health (NIH) R01 HL124986.References
[1] Pinhu, et al. Lancet. 361:332–40 (2003). [2] Tremblay et al. J. Clinical Investigations. 99(5):944-952 (1997). [3] Cereda M, et al. Anesthesiology 2016;124:121–131. [4] Kadlececk S, et al. The 24th Annual Meeting of ISMRM 2016. [5] KENNEDY TP, et al. anesth. Analg. 1989;69:87–92. [6] Shaghaghi et. al., NMR in biomedicine, 27(8):939-947 (2014).Figures
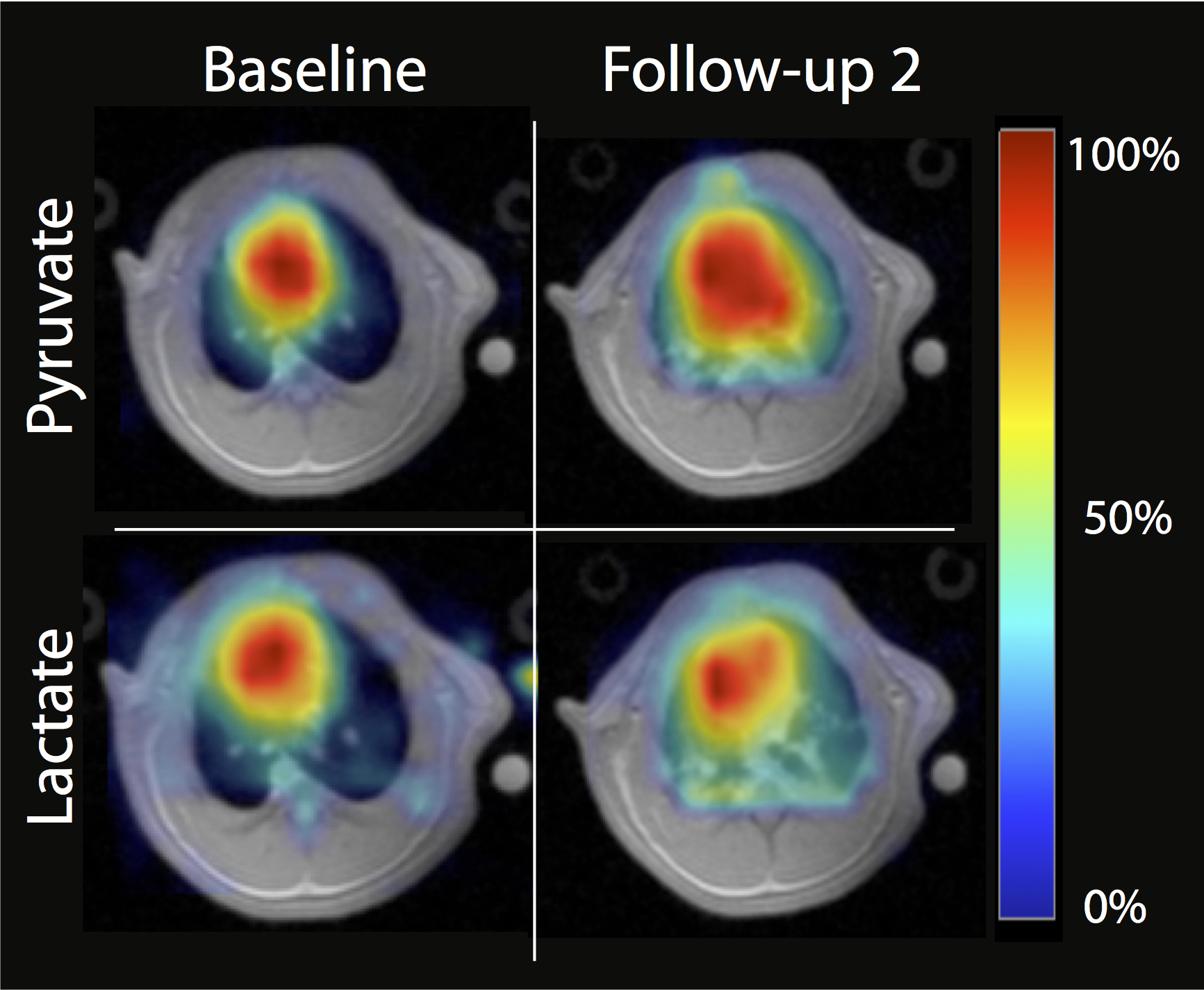
Lactate
and Pyruvate maps in a rat before and after the injury and 4 hours after
non-protective ventilation.
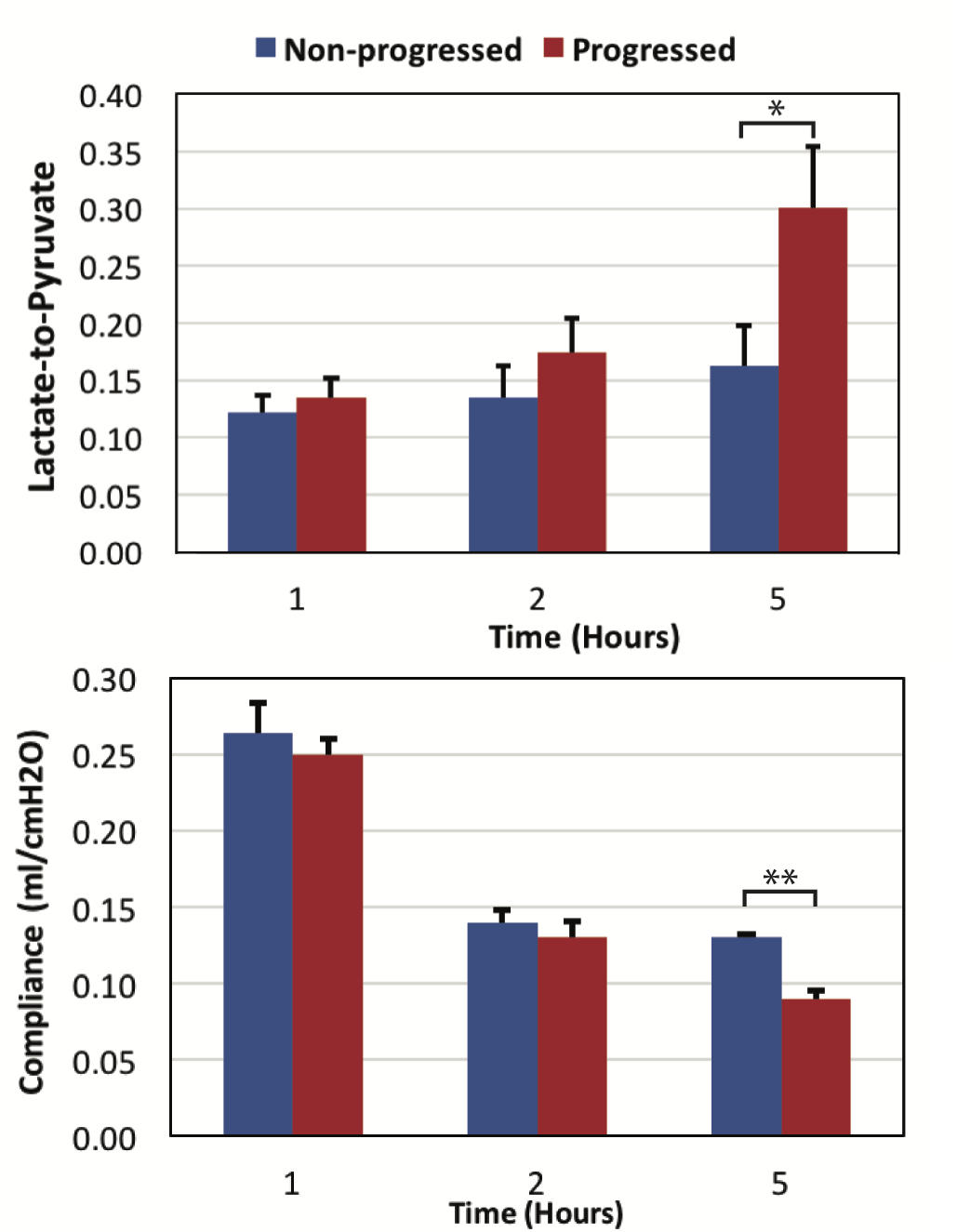
(Top) average lactate to pyruvate and (bottom) pulmonary compliance of the lungs in two cohorts as a function of time (* p < 0.05, ** p < 0.01)