2983
Treatments in chronic liver disease induced hepatic encephalopathy: a longitudinal in vivo 1H MRS study of brain metabolism using rifaximin1Laboratory for Functional and Metabolic Imaging, Center for Biomedical Imaging, Ecole polytechnique Fédérale de Lausanne, Lausanne, Switzerland, 2Center for Biomedical Imaging(CIBM), Ecole Polytechnique Fédérale de Lausanne, Lausanne, Switzerland, 3Service of Biomedicine, University Hospital of Lausanne, Lausanne, Switzerland, 4Swiss Center for Liver Disease in Children, Department of Pediatrics, University Hospitals Geneva, Geneva, Switzerland, 5Laboratory for Functional and Metabolic Imaging (LIFMET) & Center for Biomedical Imaging (CIBM), Ecole polytechnique Fédérale de Lausanne, Lausanne, Switzerland
Synopsis
Hepatic encephalopathy (HE) is a severe complication of chronic liver disease (CLD). Treatments for HE have focused on reducing plasma ammonia levels implicated in HE pathogenesis. The antibiotic rifaximin reduces the production of gut ammonia which is considered to be the main toxin in CLD-induced HE. Rifaximin is commonly used in the treatment of HE and has been shown to reduce the frequency of HE episodes, but the molecular mechanisms behind this effect are unknown. We assessed, in vivo and longitudinally, the effect of rifaximin on brain metabolites in bile duct ligated rats using high-field proton Magnetic Resonance Spectroscopy.
Introduction
Hepatic encephalopathy (HE) is a severe complication of chronic liver disease (CLD). Treatments for HE have focused on reducing plasma ammonia (NH4+) levels implicated in HE pathogenesis. The non–absorbable antibiotic rifaximin inhibits the division of colonic bacteria responsible for urea deamination, reducing the production of gut ammonia which is considered to be the main toxin in CLD-induced HE. In humans, rifaximin has been shown to reduce the frequency of HE episodes1, but the molecular mechanisms behind this effect are unknown. Therefore, our aim was to assess, in vivo and longitudinally, the effect of rifaximin on brain metabolites in bile duct ligated (BDL) rats using high-field proton Magnetic Resonance Spectroscopy (1H-MRS).Methods
Adult Wistar rats (n=8) underwent bile duct ligation, which induced chronic HE2,3. They were scanned before BDL (week0) and at weeks 2,4,6,8 after surgery. Rifaximin was administered orally twice daily (15.7mg/kg/day) starting 2 weeks after BDL-surgery (‘week2’).
In vivo 1H MRS was performed on a 9.4T MRI system (Varian/Magnex Scientific) using a home-built 14 mm diameter quadrature 1H coil as a transceiver. Metabolites evolution was studied in the hippocampus due to its role in memory, a neurologic symptom in HE and in cerebellum due to the decline of cerebellum-associated functions during HE in patients with CLD.4 Two voxels placed in the hippocampus (2x2.8x2mm3) and cerebellum (2.5x2.5x2.5mm3) were measured using SPECIAL5 sequence (TE=2.8ms, TR = 4000ms, 160 averages). First and second order shims were adjusted using FASTMAP (linewidth=9-11Hz in hippocampus and 15-17Hz in the cerebellum). Metabolite concentrations were estimated using LCModel and water as internal reference. Plasma measurements of NH4+, bilirubin, were also performed at week 0,2,4,6 and 8. Open field test was performed at week 4, 6 and 8 to evaluate motor activity as a marker of HE severity6. The results were compared to a group of our previously published BDL non-treated rats (n=26)7.
Results and discussion
All rats displayed the characteristic rise in serum bilirubin, regardless of treatment group. There was a trend toward slightly lower plasma ammonia in rifaximin treated animals (Fig.1).
1H spectra exhibited a very good SNR throughout the study, allowing easy separation of Gln from Glu (Fig.2). As can be seen in Fig.2, the characteristic pattern of chronic HE is the gradual increase of brain Gln as a result of ammonia detoxification by glutamine synthetase enzyme. This increase is followed by a decrease in Ins, Tau, tCho as an osmotic answer.
Overall, there was no significant difference in longitudinal neurometabolism between the treated and untreated groups (Fig.3). As shown in Fig.4, in both groups a gradual increase in Gln is observed , followed by the decrease in Ins, which was more pronounced in the treated group (-40%, p<0.001). tCho (GPC+PCho) showed a small decrease at week8 in the two groups. Cr, a metabolite known for its role in energy metabolism and recently reported to participate in osmoregulation and neuroprotection8,9 showed a similar decrease in both groups at week8 ( ̴̴12%). Regarding the neurotransmitters, Glu and Asp showed a decrease at week8 in both groups (7-12% and 25-70% respectively, p<0.05). Differences among other brain metabolites are presented in Fig.3.
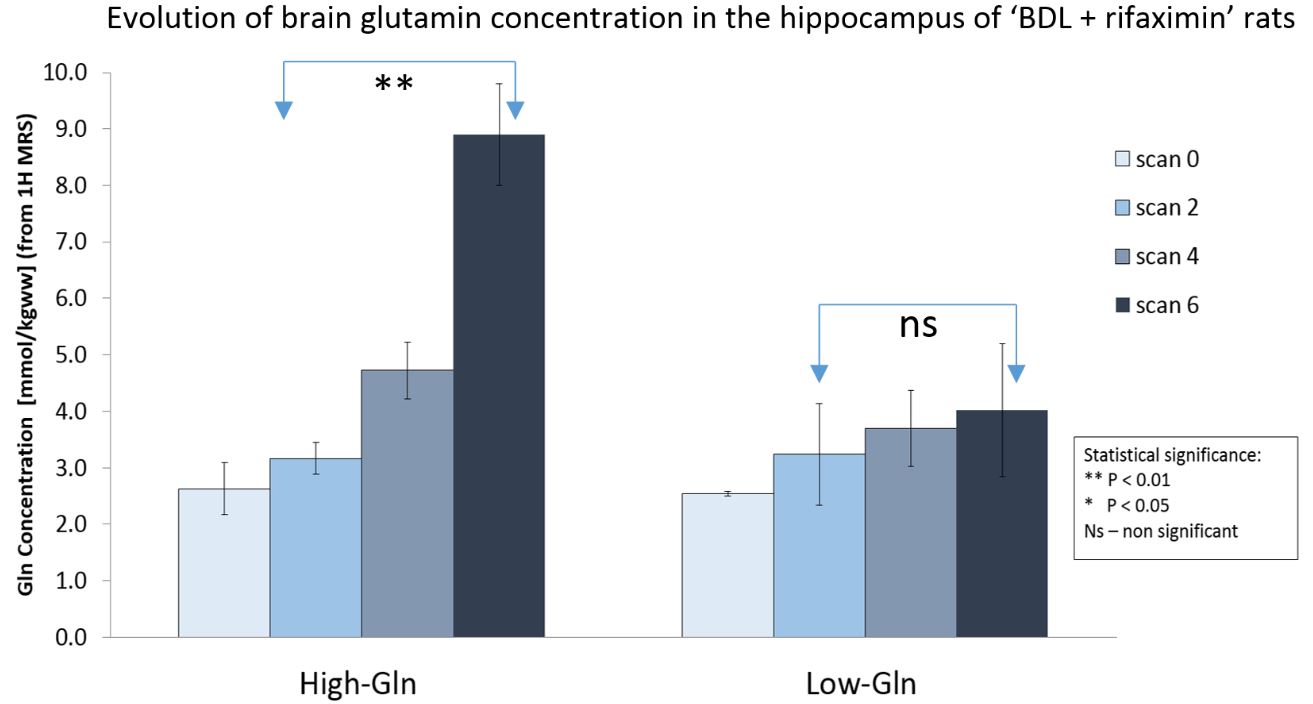
However, when analyzing the rifaximin treated group in detail, we observed two different sub-groups at week6: 4/8 of rats displayed a mild glutamine (Gln) increase at week6 vs week2 (+25±15%) while the other 4 showed a greater Gln increase (+185±55%,Fig.5), akin to untreated BDL rats. This may suggest that rifaximin contributes to reduce Gln level in a subset of rats in early stages of HE, as shown in human studies1. As expected, the decrease of other brain osmolytes (Ins, Tau, tCho) was lower for the group with a lower Gln increase. 6 weeks after surgery, glutamate showed no significant longitudinal changes in the ‘BDL+rifaximin’ rats while in the BDL rats there was 10% decrease (p=0.014).
In the rifaximin treated group, cerebellum displayed already at week6 a higher Gln concentration (+200% compared to week0) and compensatory osmolyte decrease than in hippocampus. The decrease in Tau, involved in osmoregulation, was significantly stronger in cerebellum than in hippocampus already at 6 weeks after surgery (-28%, p<0.01, Fig.4C).
Conclusion
Our preliminary results suggest that rifaximin may help reducing Gln level in early stages of HE, but further studies are clearly required to assess the impact of rifaximin on the neurometabolic profile of BDL rats and to assess its therapeutic role. The clinical implications of these findings are potentially far-reaching given that rifaximin is a commonly used antibiotic in the treatment of HE, generally safe and well-tolerated.Acknowledgements
Supported by CIBM of the UNIL, UNIGE, HUG, CHUV, EPFL, the Leenaards and Jeantet Foundations.References
1Bajaj et al, Ap&T 2016 ; 2Biecker et al, J Pharmacol Exp Ther 2005; 3Butterworth et al, Liver Int 2009; 4Singh, S. & Trigun, S.K. Cerebellum 2010; 5Mlynárik et al, Magn Reson Med 2006; 6Leke et al, Plos one 2012; 7Cudalbu et al, Metab Brain Dis 2012 ; 8Rae, NeurochemRes 2014; 9Braissant, MolGenetMetab 2010Figures
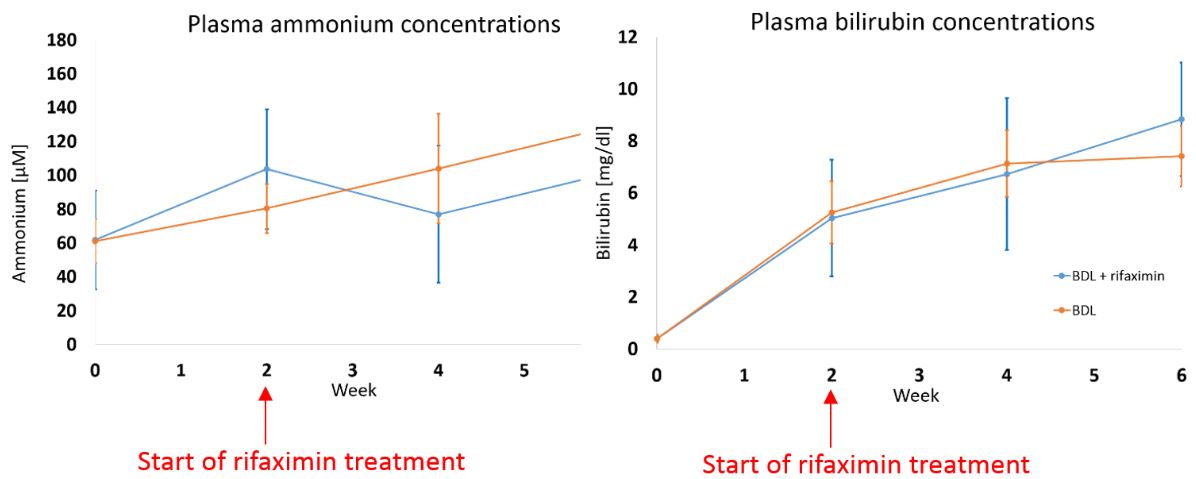
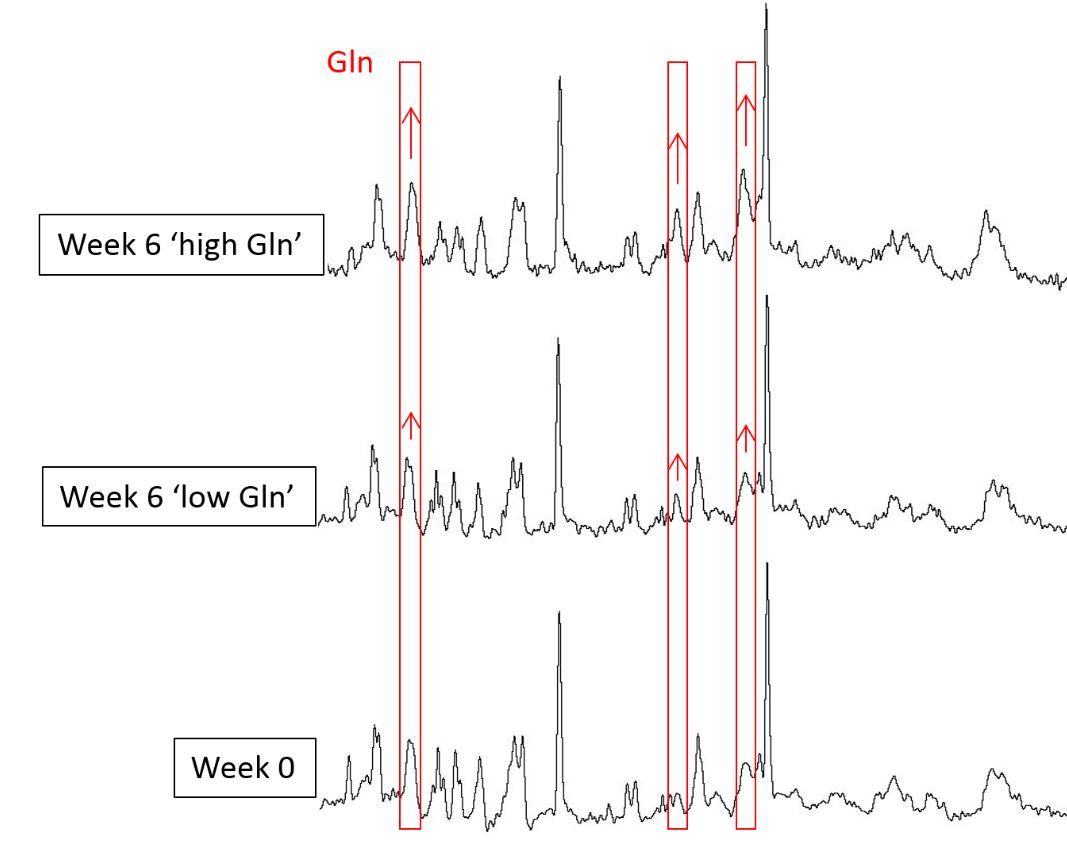
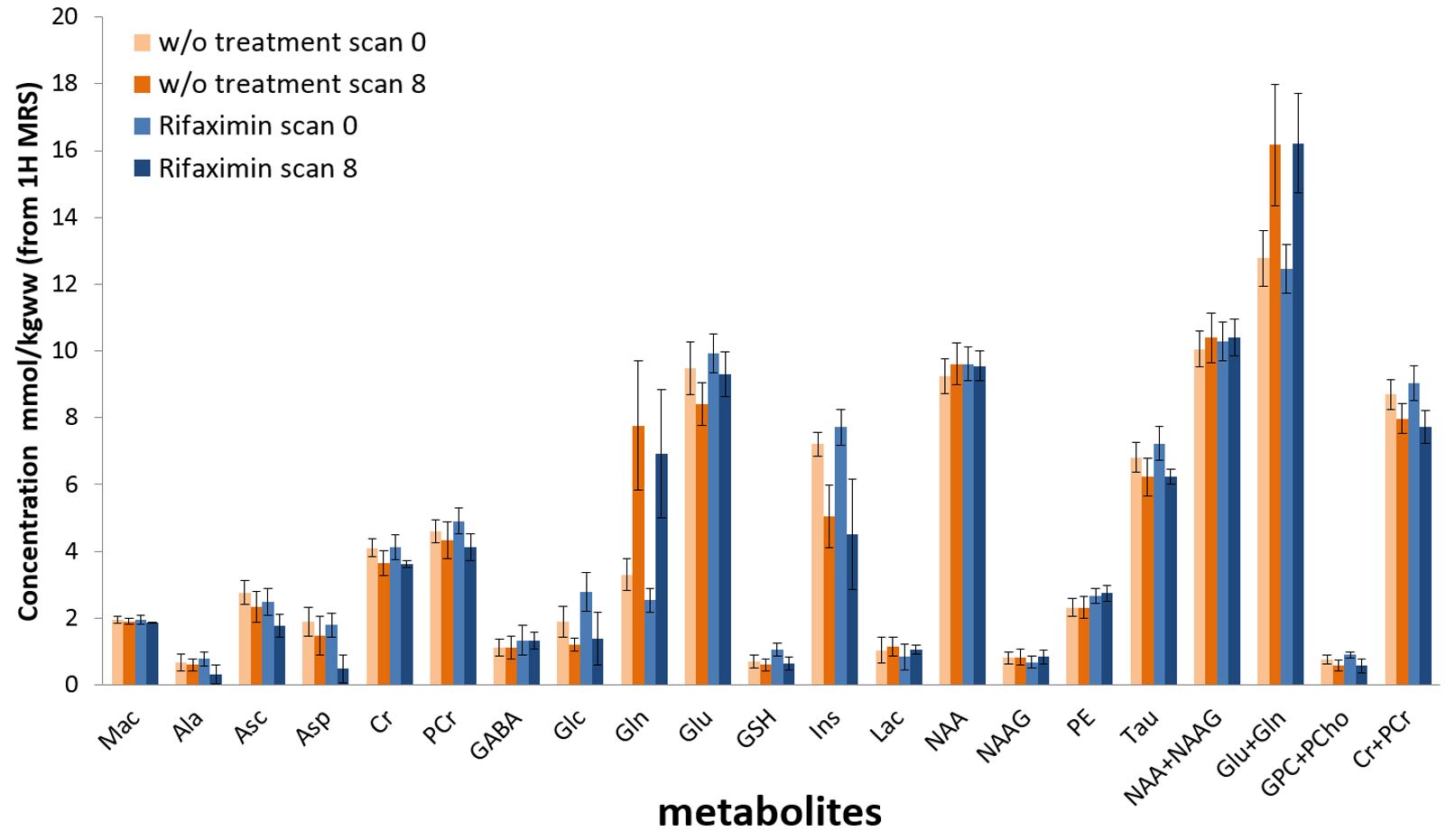
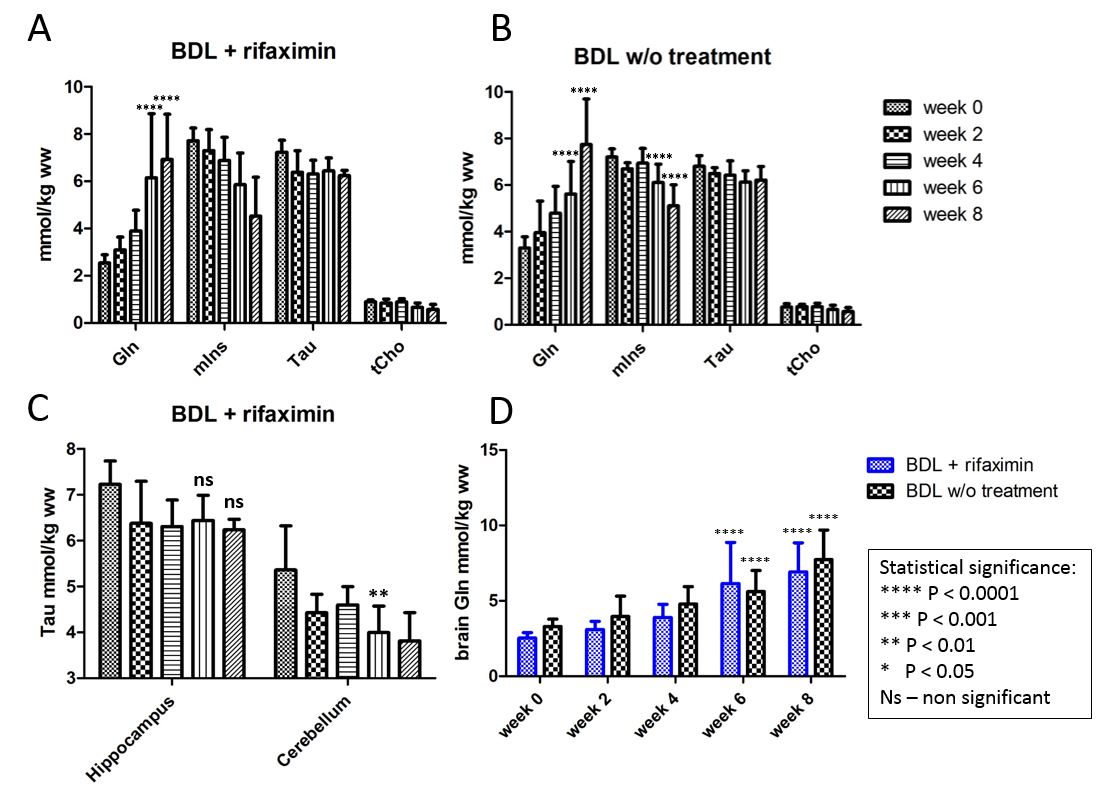
Fig.4 A,B- Longitudinal evolution of the main brain osmolytes in the rifaximin treated group and the group without treatment.
C- Evolution of taurine in hippocampus and cerebellum of the rifaximin treated group of rats.
D- Differences in brain Gln between rifaximin treated and non-treated animals.
Two-way
ANOVA statistical tests were performed using GraphPad Prism software. Statistical significance shows the comparison with week 0.