2906
Evaluation of 4D-T2w MRI methods for lung radiotherapy treatment planning with application to an MR-linac1Joint Department of Physics, The Institute of Cancer Research and The Royal Marsden NHS Foundation Trust, London, United Kingdom, 2CR-UK Cancer Imaging Centre, The Institute of Cancer Research, London, United Kingdom, 3Medical Physics in Radiology, German Cancer Research Center (DKFZ), Heidelberg, Germany
Synopsis
Due to enhanced soft-tissue contrast, 4D-T2w MRI could improve lung tumour target delineation in radiotherapy compared with 4D-CT; reducing planning margins and dose to healthy tissue for treatments on an MR-linac. We have developed a method for generating 4D-T2w MRI, where 3D-T2w MRI is warped using motion vector fields; calculated by image-registration between respiratory phases of 4D-T1w MRI (the MVFP method). Here, 4D-T2w MRI calculated with MVFP and with amplitude-binning of continuously acquired 2D-T2w MRI, are compared. 4D-T2w MRI from the MVFP method exhibited higher image quality and geometrical fidelity than the 2D-binning scheme, but displayed possible motion under-estimation.
Purpose
We have developed a method for calculating 4D-T2w MRI, the motion vector field projection (MVFP) method, and compared it to 4D-T2w MRI generated by a 2D-binning method in the context of radiotherapy treatment planning of lung cancer for MR-Linac1 based treatment. Due to its superior soft-tissue contrast, delineation on 4D-T2w MRI instead of 4D-CT could reduce planning margins and thus dose delivered to healthy tissue.
Methods
4D-T2w MRI was obtained using the MVFP method and also a slice-selective 2D-binning method, similar to Liu et al2, for one lung cancer patient and two healthy volunteers.
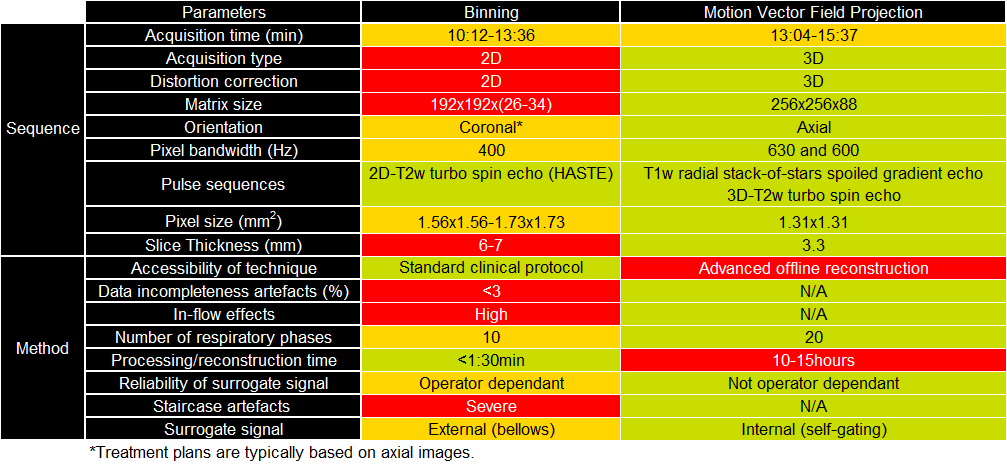
In the MVFP method, motion vector fields are calculated by performing deformable image registration between the respiratory phases of an offline reconstructed3 4D-T1w volume. 4D-T2w MRI is then generated by warping 3D-T2w MRI employing the motion vector fields. Detailed acquisition parameters for both methods can be found in Figure 1. In the 2D-binning method, subjects were scanned with a 2D-T2w turbo spin echo sequence at 1.5T (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany), whilst recording a respiratory bellows signal using the Siemens physiological monitoring unit. 4D-T2w MRI was obtained by retrospective sorting of the images into ten bins based on the amplitude of the respiratory surrogate. Amplitude bins contained the same number of acquired images. If for a particular slice multiple images were assigned to the same bin, the image with best matching surrogate signal was selected.
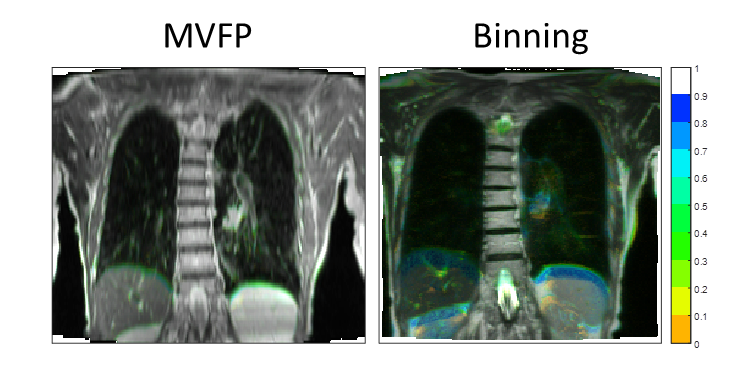
The two 4D-T2w MRI approaches were compared regarding the range of captured motion for one coronal slice across all respiratory phases by using colour intensity projection images4 (CIPs) and the diaphragm position obtained from an edge-detection algorithm. CIPs were calculated by combining the maximum, mean and minimum intensity projections into a red-green-blue colour map. Edge-detection was facilitated by fitting an error function to the diaphragm boundary.
Results
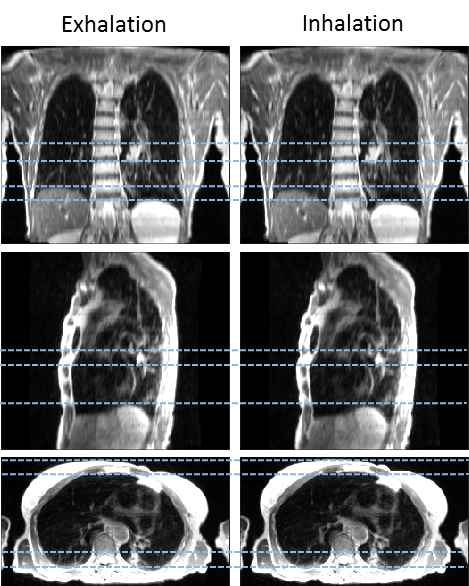
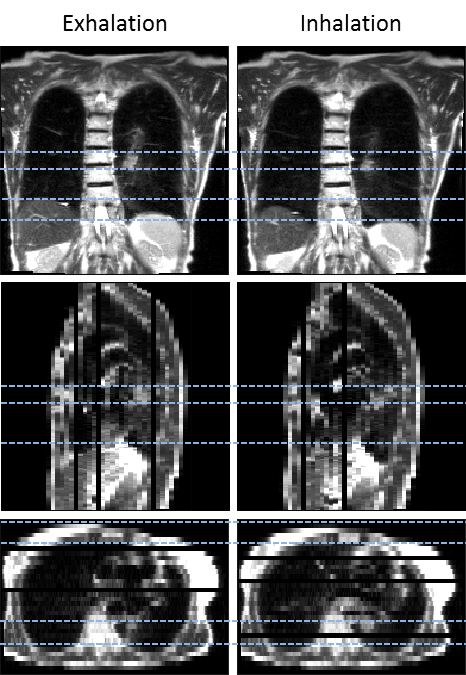
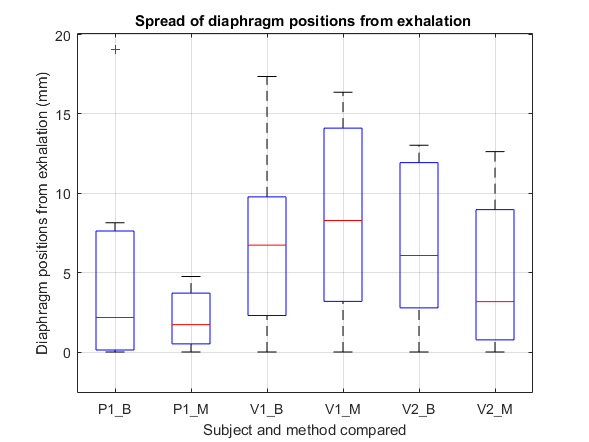
Figures 2 and 3 show 4D-T2w MRI obtained for the patient using the MVFP and 2D-binning methods. Figure 1 displays a comparison between the two methods. 4D-T2w MRI calculated by the MVFP method exhibited higher spatial resolution, twice the number of respiratory bins and a larger FOV compared to the 2D-binning method, which is limited by both SNR and acquisition time. While the MVFP method employs a 3D acquisition, enabling a full 3D distortion correction, the 2D-binning method is restricted to a 2D in-plane distortion correction. Unlike the MVFP method, results from the 2D-binning method suffer from: staircase artefacts due to greatly non-isotropic voxel sizes; incompleteness artefacts, where a slice was not acquired in all respiratory phases; and in-flow effects, associated with 2D slice-selective excitation. However, the MVFP method requires a long reconstruction time. Figure 4 shows example CIPs for the patient. The 2D-binning CIP displays an extreme respiratory phase as well as increased movement in the external boundary of the body, compared to the MVFP CIP. In Figure 5, the spread of diaphragm positions centred at exhalation is shown. Median diaphragm positions are consistent to <3mm for all subjects. The total range of diaphragm positions are consistent to <1mm for the volunteers, but shows a large displacement (outlier) >14mm for the patient.Discussion
4D-T2w MRI calculated with the MVFP method could be more suitable for treatment planning of lung cancer for the MR-linac than 4D-T2w MRI obtained from the 2D-binning method, as it exhibits: finer spatio-temporal resolution, higher geometrical fidelity (3D distortion correction) and reduced image artefacts (staircase, data incompleteness and in-flow). Additionally, the MVFP method enables a larger FOV to be acquired, allowing clinicians to more accurately determine the external body contour, crucial for accurate dose calculations. However, the MVFP method could over-regularise motion, as indicated by the reduction of external boundary motion observed in the MVFP CIP and also the deeper inspiration highlighted in the 2D-binning CIP. While those differences could also be explained by breathing variability or patient motion, over-regularisation could result in an underestimation of necessary radiotherapy planning margins. Compared to the MVFP method, the 2D-binning method requires a short processing time, and therefore could be more suitable for implementing 4D-T2w MRI on the MR-linac. However, there is scope to optimise the MVFP method and to reduce processing time, which alongside the above-mentioned advantages could enable the MVFP method to be applied clinically as the method of choice.Conclusion
4D-T2w MRI obtained using the MVFP workflow exhibits: finer spatio-temporal resolution, higher geometrical fidelity, full FOV coverage over respiratory cycles and reduced image artefacts when compared to 4D-T2w MRI generated by a 2D-binning scheme. However, the 2D-binning method requires a short processing time and may capture a more representation range of motion.Acknowledgements
We acknowledge NHS funding to the NIHR Biomedical Research Centre and the Clinical Research Facility at The Royal Marsden and The Institute of Cancer Research and CR-UK Cancer Imaging Centre grant C1060/A10334. We are grateful to Alto Stemmer of Siemens Healthcare, Erlangen, Germany for providing us with WIP sequence #528R. Andreas Wetscherek is funded by CR-UK project grant C33589/A19727. Joshua Freedman is supported under CR-UK Non Clinical Centre grant CRM089X.References
1. Raaymakers BW, Lagendijk JJ, Overweg J et al. Integrating a 1.5 T MRI scanner with a 6 MV accelerator: proof of concept. Phys Med Biol. 2009;54(12):N229
2. Liu Y, Yin FF, Czito BG, et al. T2-weighted four dimensional magnetic resonance imaging with result-driven phase sorting. Med Phys. 2015;42(8):4460-71.
3. Rank CM, Heußer T, Buzan MT, et al. 4D respiratory motion-compensated image reconstruction of free-breathing radial MR data with very high undersampling. Magn Reson Med. 2016;doi:10.1002/mrm.26206.
4. Cover KS, Frank JL and Suresh S. Color intensity projections: A rapid approach for evaluating four-dimensional CT scans in treatment planning. Int J Radiat Oncol. 2006;64(3):954-961.
Figures