2904
Prognostic Characterization of Prostate Cancer from Benign Tissue MRSLeo L. Cheng1, Emily A. Decelle2, Johannes L Kurth2, Shulin Wu3, Taylor L. Fuss2, Lindsey A. Vandergrift2, Elita M. DeFeo2, Elkan F. Halpern2, Matthias L Taupitz2, W. Scott McDougal2, Aria F. Olumi2, and Chin-Lee Wu2
1Molecular Pathology, Massachusetts General Hospital, Charlestown, MA, United States, 2Massachusetts General Hospital, Charlestown, MA, United States, 3Massachusetts General Hospital, Boston, MA, United States
Synopsis
While serum prostate specific antigen (PSA) testing improved early detection of prostate tumors, implementation of this tool also created a large patient population in which identified cancer lesions were actually indolent. For patients who choose to undergo prostatectomy, cancer aggressiveness can only be determined by post-procedure pathology analysis of cancerous tissue. Additionally, cancer recurrence predictions are often unreliable. As an alternative method to aid decisions regarding treatment, we sought to develop MRS tools which can predict cancer aggressiveness based on the novel use of histologically benign (Hb) tissue.
Introduction
The clinical challenge of prostate cancer (PCa) arises due to the fact that over 70% of patients diagnosed by the gold standard of serum prostate specific antigen (PSA) screening will have an indolent form of cancer with little effect on their well-being. More aggressive cancer which does harm well-being is found in about 12% of PSA-diagnosed patients. For the patients in this group who do undergo prostatectomy, tumor grade can only be determined post-operatively. Furthermore, current predictive nomograms are fraught with uncertainty about likelihood of cancer recurrence. Under the hypothesis that metabolomic fields within cancerous tissue can cause metabolite delocalization into neighboring benign tissue, we aimed to develop biomarkers to distinguish indolent from aggressive PCa using histologically benign (Hb) tissues of PCa patients. Implementation of such a diagnostic could prevent overtreatment and create more individualized therapy plans.Methods
After radical prostatectomy, 365 tissue samples were collected from 158 cancerous prostates. They were snap-frozen in liquid nitrogen <45 minutes after radical prostatectomy and stored at -80oC until MRS analyses. Overall experimental design for characterization of tissue is diagrammed in Figure 1. Intact tissue MRS. Tissue scans were conducted with high-resolution magic angle spinning on a Bruker AVANCE 600MHz spectrometer. Samples were weighted (~10mg) and placed into a 4mm rotor with plastic inserts to create a 10µl sample space; 1.0µl D2O was added for field locking. Spectra were recorded at 4ºC with a repetition time of 5s, and a rotor-synchronized DANTE protocol conducted with spinning at both 600 and 700Hz. Data were analyzed using AcornNMR-Nuts with relative intensities obtained from integrated intensities normalized by the spectral intensity between 0.5 and 4.5ppm. Quantitative histopathology. Tissue was processed and analyzed by traditional histopathology. Quantification of volume percentages of pathological features and PCa/Hb categorization of tissue was performed by a pathologist.Results
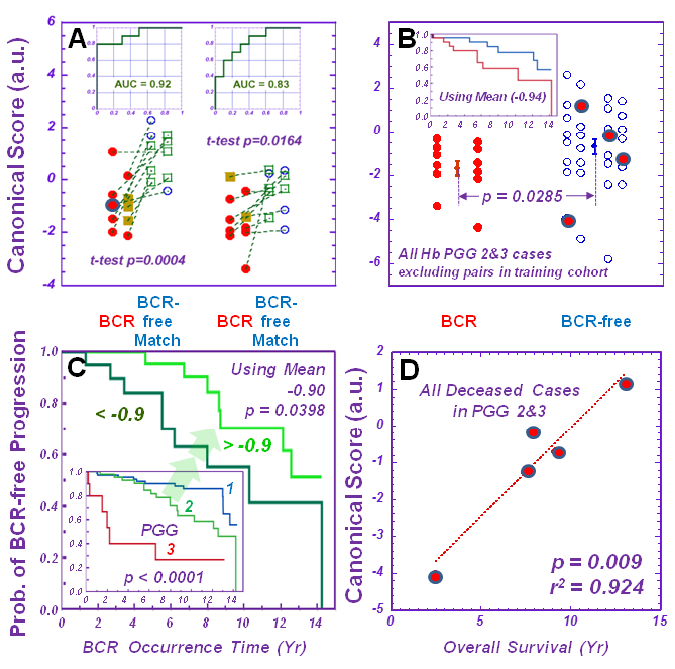
Analyses indicate the ability of MRS to determine cancer aggressiveness. The 3.60ppm spectral region in Hb prostatectomy tissue can differentiate between PCa prognostic grade group (PGG)1&2 and PGG3&4 groups, with an overall accuracy of 73% and 71% for the training and testing cohorts. Tumor groups, specifically pT=IIab and pT=IIac, can also be distinguished using the lipid spectral region of 0.93-0.96ppm. Further analysis showed that the 3.60ppm region and principal component (PC) 4 could distinguish a subgroup of low malignant potential from the main group. Application of these PC4 parameters to a testing cohort showed that 10 of 58 (17%) of low aggressive cases could be distinguished among all 72 (14%) cases. Lastly, MRS measurements of Hb tissue help predict tumour biochemical recurrence (BCR). Principal components and canonical analyses calculated from 36 spectral regions of ten pairs of BCR and non-BCR cases with the training cohort can differentiate BCR from non-BCR cases within the testing cohort with an accuracy of 83% (Figure 2A). Given that the canonical score was comprised primarily of PGG 2 and 3 cases, applying the canonical score calculations onto the PGG 2 and 3 cases resulted in a statistically significant differentiation between BCR and non-BCR cases (Figure 2B). Within the PGG 2 group only, the BCR discriminant canonical values can further differentiate the group into two (Figure 2C) according to Kaplan-Meier analysis. The canonical score also linearly correlate with patient survival time (r2 = 0.924) (Figure 2D).Discussion and Conclusions
Where pathological analysis of a benign core might present a false negative due to the heterogeneity of PCa, the ability of the spectral region to distinguish between cancer grades could enable MRS to detect of aggressive forms of cancer when pathology fails to do so. Currently tumor grade can only be determined after radical prostatectomy, but the capability of the spectral regions in Hb tissue to determine tumor aggressiveness could inform treatment decisions prior to surgical intervention. Even with imperfect characterizations, identification of a distinct low malignancy potential group could better inform the therapy plan for 110,000 patients annually worldwide. Nomograms today remain incapable of differentiating between matched cases, so the ability of canonical scores from our matched BCR and non-BCR cases to predict likelihood of cancer recurrence and survival time highlights their potential as a clinical tool. These findings demonstrate the ability of MRS-measured metabolomic fields in Hb tissue to detect biochemical changes, and, as a result, determine disease aggressiveness. We present their potential utility as diagnostic tools to better inform treatment decisions in the PCa clinic.Acknowledgements
Authors acknowledge support by PHS NIH grants CA115746, CA115746S2, and CA162959 and the A. A. Martinos Center for Biomedical Imaging.References
No reference found.Figures
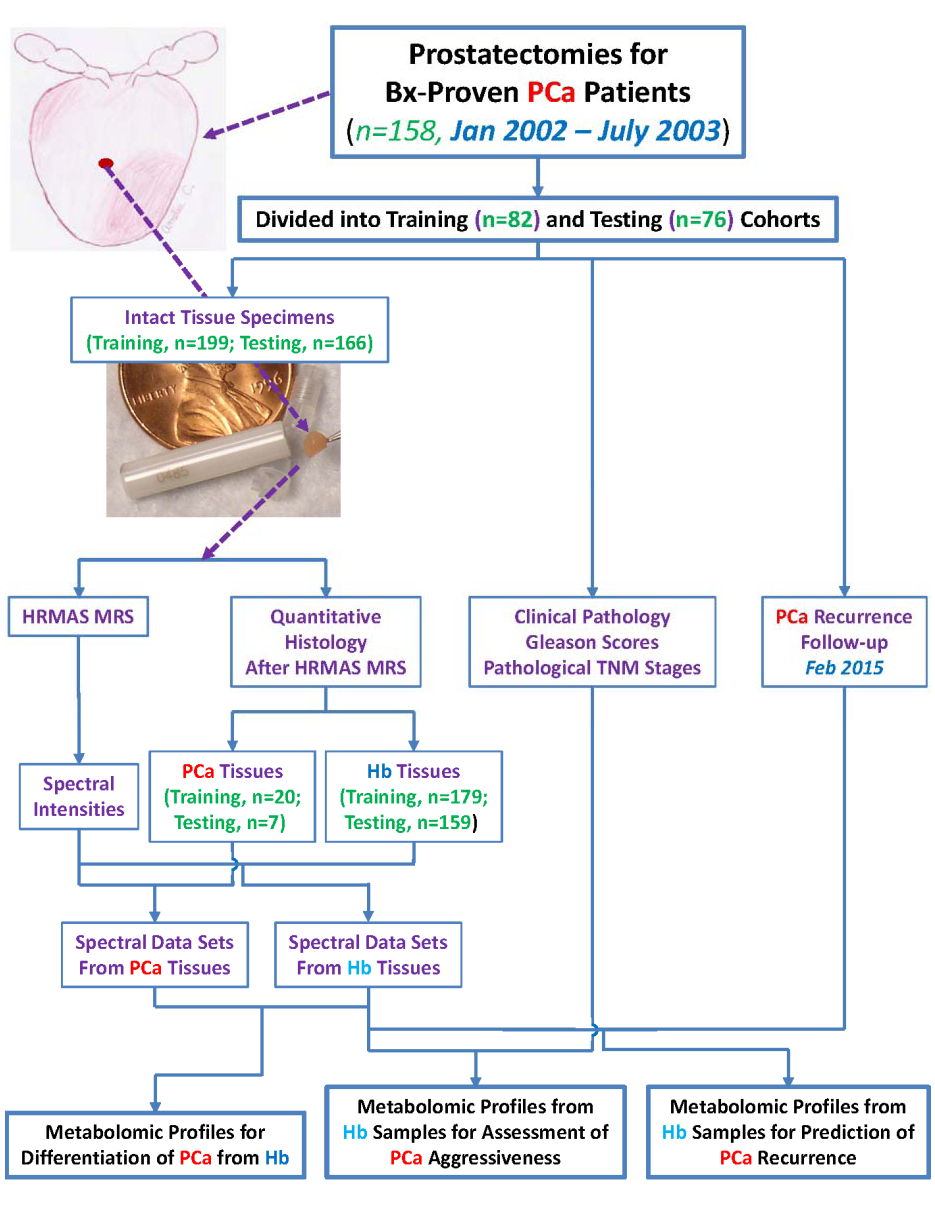
Experimental
design to generate metabolomic profiles for (a) differentiation between PCa and
Hb tissue, (b) determination of cancer aggressiveness, and (c) prediction of
PCa recurrence.
Prediction
of PCa potential at the time of surgery.