2887
Interaction of Pulmonary Regurgitation Flow and Myocardial Motion Velocity in Patients with Repaired Tetralogy of Fallot1Department of Biomedical Engineering and Environmental Sciences, National Tsing Hua University, Hsinchu, Taiwan, 2Department of Radiology Kaohsiung, Kaohsiung Veterans General Hospital, 3Department of Medical Imaging Taipei, National Taiwan University Hospital
Synopsis
In this study, we measured pulmonary regurgitation fraction and three-directional myocardial wall motion velocities to establish indices for characterizing cardiac function in patients with repaired tetralogy of Fallot (rTOF). We aim to reveal the interaction of pulmonary regurgitation fraction and myocardial motion velocity and thereby to speculate the myocardial damage in rTOF patients. In conclusion, the pulmonary RF displayed
Introduction
A previous study reported the correlation between pulmonary regurgitation and right ventricular end-diastolic volume as well as RV ejection fraction in patients with repaired tetralogy of Fallot.1 However, the association between pulmonary regurgitation fraction (RF) and myocardial function is less discussed. In this study, we measured pulmonary RF and three-directional myocardial wall motion velocities to establish indices for characterizing cardiac function in rTOF patients. The purpose of this study is to reveal the interaction of pulmonary RF and myocardial motion velocity and thereby to speculate the myocardial damage in rTOF patients.Method
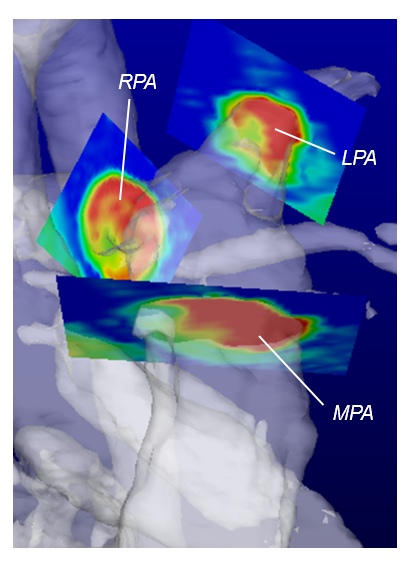
The study population included 15 rTOF patients (21.7±3.2 y/o; male/female: 11/4) and 20 healthy controls (21.4±0.8 y/o; male/female: 13/7). All images were acquired on a 3.0-Tesla MR scanner (Trio with Tim or Skyra, Siemens, Erlangen, Germany). A 4D flow MRI adopted fast low angle shot (FLASH) sequence was used to acquire pulmonary flow velocity. A black-blood FLASH sequence was performed to acquire myocardial velocity information in basal, mid-ventricular, and apical short-axis slices, acquiring 80-90% of the R-R interval (TR= 26 ms, TE= 4.2 ms, slice thickness= 6 mm, flip angle= 7°, pixel size= 1.17x1.17mm2). The navigator gating and prospective ECG triggering were used to synchronize with respiratory and cardiac motion, respectively. The left ventricular (LV) and right ventricular (RV) myocardium were divided into 16 and 10 segments. LV and RV longitudinal (Vz) as well as radial (Vr) myocardial velocities were computed. The 4D flow data was reconstructed by EnSight for visualizing the 3D angiogram of pulmonary arteries. Three 2D planes for calculation of flow velocity were prescribed perpendicular to the main pulmonary artery (MPA), left pulmonary artery (LPA), and right pulmonary artery (RPA). Main pulmonary artery plane was placed 2 cm from the bifurcation. Left/right pulmonary artery plane was placed 1 cm from the bifurcation, as shown in Figure 1. Statistical analysis was performed to quantify the pulmonary RF and to assess its correlation with myocardial velocities.Results
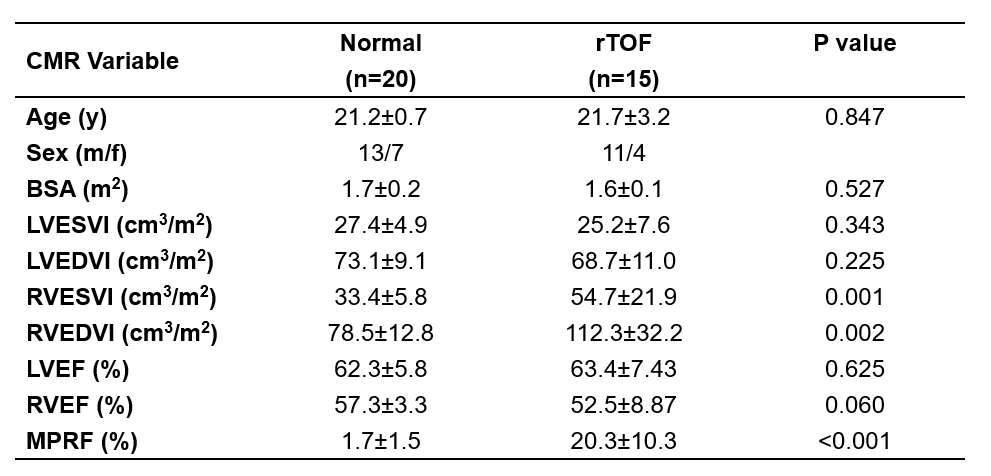
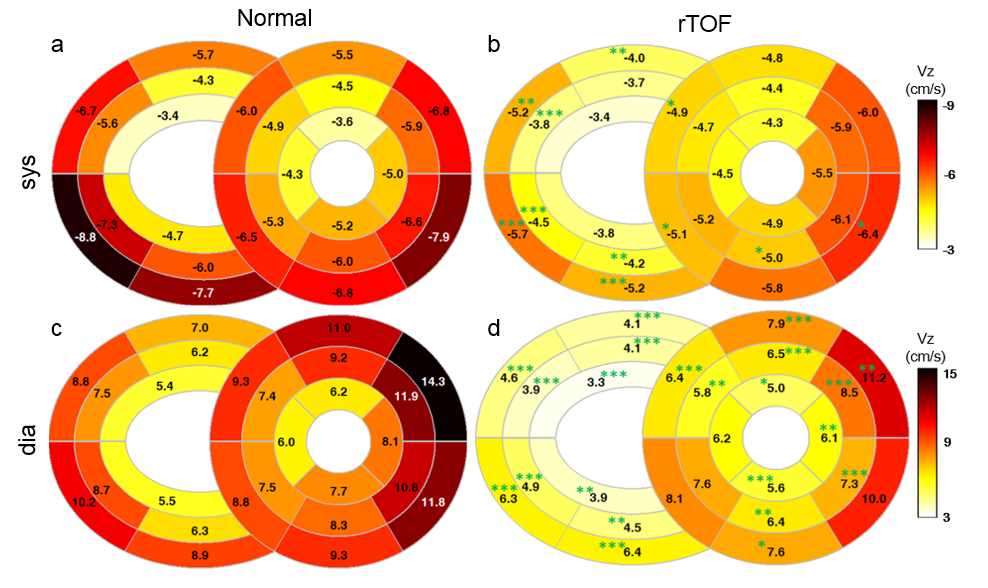
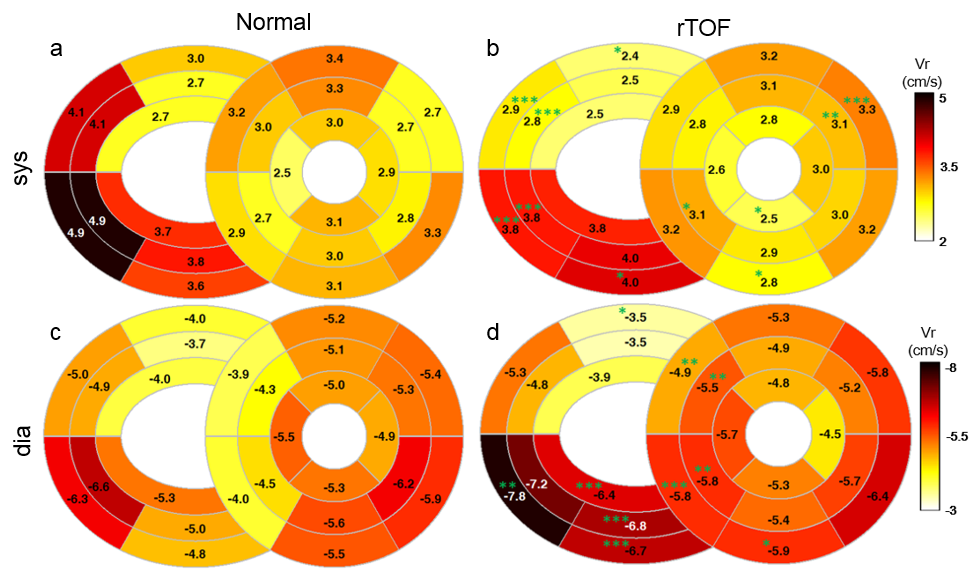
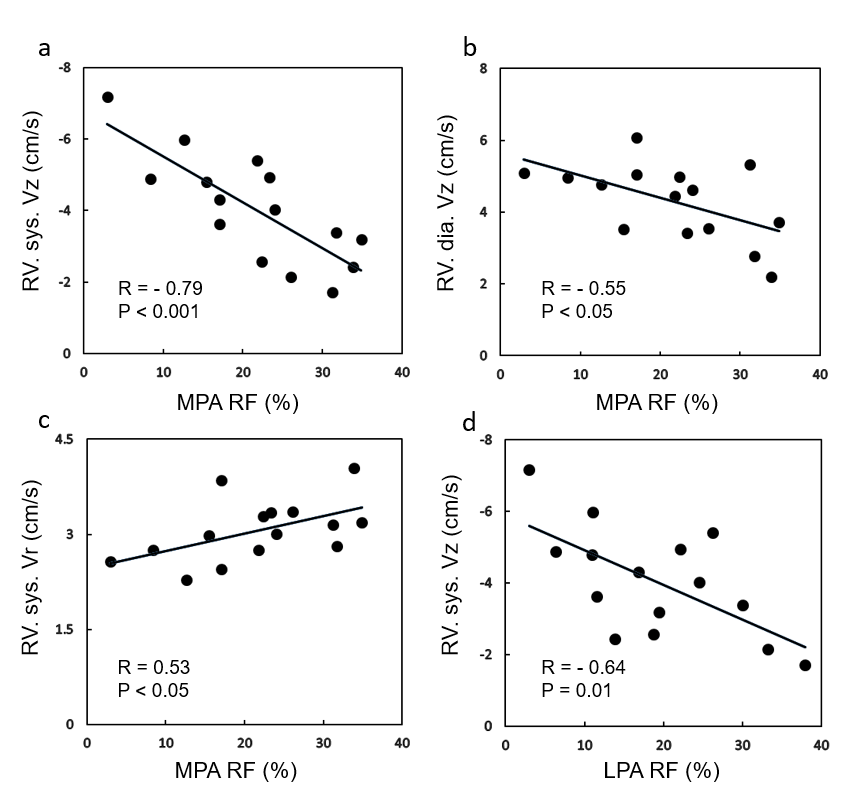
Table 1 summarizes the characteristics and cardiac MR parameters of study population. There was no significant difference in age, BSA, LV ejection fraction (EF), and RVEF between patient and normal groups. Patients showed significant higher right ventricular end systolic volume index (54.7±21.9 vs. 33.4±5.8, P=0.001) and right ventricular end diastolic volume index (112.3±32.2 vs. 78.5±12.8, P=0.002) than normal group, indicating that patients were with the presence of dilated RV. The patients also displayed significant higher pulmonary RF in MPA than normal group (20.3±10.3% vs. 1.7±1.5%, P<0.001). In Figure 2, compared with normal controls, patients presented significantly decreased systolic Vz on RV free wall and decreased diastolic Vz both on RV and LV segments. In respect of Vr, rTOF patients exhibited significantly reduced systolic Vr on RV free wall and increased Vr on RV inferolateral wall as well as on LV septum (Figure 3). Figure 4 displayed the correlation between RV myocardial velocities and pulmonary RF in rTOF patients. The MPA RF displayed significant negative correlation with RV Vz in systole (R= -0.79, P<0.001) and in diastole (R= -0.55, P<0.05). Further, The MPA RF presented a positive correlation with systolic Vr (R= 0.53, P<0.05). We also observed a high negative correlation between LPA RF and systolic Vz (R= -0.64, P=0.01).Discussion and Conclusion
In this study, we quantified the myocardial velocities in RV and LV as well as the pulmonary RF for rTOF patients and controls group. In the previous study, the endocardium was considered to be more sensitive to pathology abnormality than epicardium.2 Babu-Narayan et al adopted late-Gd enhancement MR images and reported that increased pulmonary RF caused RV overload and myocardial fibrosis and stiffness.3 In our study, the decreased systolic and diastolic Vz in RV reflected the impaired RV contraction and relaxation. In the meanwhile, a positive correlation between RV systolic Vr and MPA RF implied that increased Vr may demonstrate a compensatory mechanism to overcome the pulmonary RF and thereby to maintain the cardiac function. Atsuko et al mentioned that the LPA presented lower distensibility and higher pulmonary vascular resistance than RPA in rTOF patients.4 In our work, we found a higher correlation between RV systolic Vz and regurgitation fraction in LPA than in RPA, implying a more sensitive response to the impaired myocardium in LPA. In conclusion, the pulmonary RF displayed negative correlation with Vz and positive correlation with Vr in the RV of rTOF patients. The analyses of pulmonary flow and myocardial motion velocity can help to comprehend the interaction between pulmonary regurgitation flow and impaired myocardium in rTOF patients, and it may provide useful information for clinical patient managements.Acknowledgements
No acknowledgement found.References
1. Geva et al. Repaired tetralogy of Fallot: the roles of cardiovascular magnetic resonance in evaluating pathophysiology and for pulmonary valve replacement decision support. Journal of Cardiovascular Magnetic Resonance. 2011, 13:9
2. Bansal et al. Longitudinal and circumferential strain in patients with regional LV dysfunction. Curr Cardiol Rep. 2013, Mar;15(3):339
3. Babu-Narayan et al. Diagnosis and Management of Adult Congenital Heart Disease Circulation. 2006, 113:405
4. Atsuko et al. Vicious circle between progressive right ventricular dilatation and pulmonary regurgitation in patients after tetralogy of Fallot repair? Right heart enlargement promotes flow reversal in the left pulmonary artery Journal of Cardiovascular Magnetic Resonance. 2016, 18:34
Figures