2884
Reducing Specific Energy Deposition in Free Breathing Balanced Steady-State Free Precession (bSSFP) Cine Imaging using Cardio-respiratory SynchronizationAmol Pednekar1,2, Benjamin Cheong3, Janie Swaab4, Melissa Andrews3, Debra Dees3, and Raja Muthupillai2
1Philips Healthcare, Houston, TX, United States, 2Baylor St. Luke's Medical Center, Houston, TX, United States, 3Diagnostic and Interventional Radiology, Baylor St. Luke's Medical Center, Houston, TX, United States, 4Department of Diagnostic and Therapeutic Radiology, Baylor St. Luke's Medical Center, Houston, TX, United States
Synopsis
Free breathing cine bSSFP sequences with minimal compromises in spatio-temporal resolution requirements are highly desirable in patients who can not hold their breath, e.g., sedated patients, patients with poor cardiopulmonary reserve, patients with arrhythmia etc. The results from this prospective clinical study of 14 clinical patients shows that a cardiorespiratory synchronized (CS) sequence can reduce specific energy deposition (0.68 ± 0.24 kJ/kg) by 40% compared to a respiratory gated (RG) sequence (1.2 ± 0.36 kJ/kg) without compromising spatial, temporal, and contrast resolution thus permitting the prescription of bSSFP cine sequences with higher spatial or temporal resolution, and coverage.
PURPOSE
To quantify the reduction in RF energy deposition of a real-time adaptive cardiorespiratory synchronized (CS) balanced Steady State Free Precession (bSSFP) sequence compared to conventional respiratory gating (RG).BACKGROUND
Despite the advantages of breath-hold cine bSSFP imaging, respiratory suspension—an essential mechanism for acquiring bSSFP cine images in the steady state —is not suitable for all patients, such as sedated patients and patients with impaired breath-holding capacity and/or cardiac arrhythmias. Therefore, it would be of clinical interest to obtain cine bSSFP images in individuals without the constraint of breath holding. Traditional approach to obviate the need for breathholding via respiratory gating (RG) imposes a significant RF energy deposition for bSSFP cine imaging, due to the uninterrupted application of high-flip angle RF pulses throughout the respiratory cycle. A respiratory triggered (RT) approach could mitigate these challenges1. In this prospective study on 14 consecutive clinical patients, we compared the specific energy deposition (SED) of a real-time adaptive, cardiorespiratory synchronized (CS) bSSFP sequence with RG sequence with identical acquisition parameters.METHODS
Fourteen consecutive patients (54(32-80)yrs, 70(58-104)hbm, 19(18-22)rpm) undergoing clinically indicated cardiac MR, provided written informed consent to participate in this IRB approved, prospective study. All imaging was performed on 1.5T(9)/3T(5) commercial MR scanners (Achieva/Ingenia, Philips Healthcare). CS sequence that performs a) respiratory synchronized drive to steady state, b) prospective cardiorespiratory synchronized cine data acquisition with arrhythmia rejection, and c) retrospective cardiac gating was implemented (Fig 1). Cine bSSFP data was acquired with CS and conventional breath-hold (BH) sequence with identical acquisition parameters (TR/TE/flip angle = 2.5-3.2ms/1.25-1.6ms/ 65°(40°,3T); acqd voxel size = 1.7-2.0×1.6-2.0×8mm3; SENSE factor = 1.3-1.9; temp resolution 40-50ms; imaging time : 6-8 RR intervals/slice) for LV function evaluation. The data acquisition and physiology log was analyzed to compute RF duty cycle, and specific energy deposition for both the sequences.RESULTS
The CS sequence ran successfully in all 14 patients. Total image acquisition time for CS (7.4±1.8 min) was significantly longer than conventional BH-SSFP (5.6±1.7 min). Reduction in SED for the CS sequence (0.68 ± 0.24 kJ/kg) compared to RG sequence (1.2 ± 0.36 kJ/kg) was statistically significant (Fig 2). The mean rate of energy deposition (kJ/kg/min) for the CS sequence was 40% lower than that of RG sequence (Fig 3). Clinical scores indicate diagnostically equivalent image quality with CS sequence as that of conventional BH techniques.CONCLUSION
The CS sequence provides the ability to prescribe multi-slice, multi-phase bSSFP sequences with significantly lower SED burden than that of RG sequence. This extends the utility of bSSFP sequences to acquire high spatial or temporal resolution images during free breathing with greater latitude in terms of RF energy deposition in sedated subjects.Acknowledgements
No acknowledgement found.References
[1] Krishnamurthy et al., JCMR, 17:1, 2015.Figures
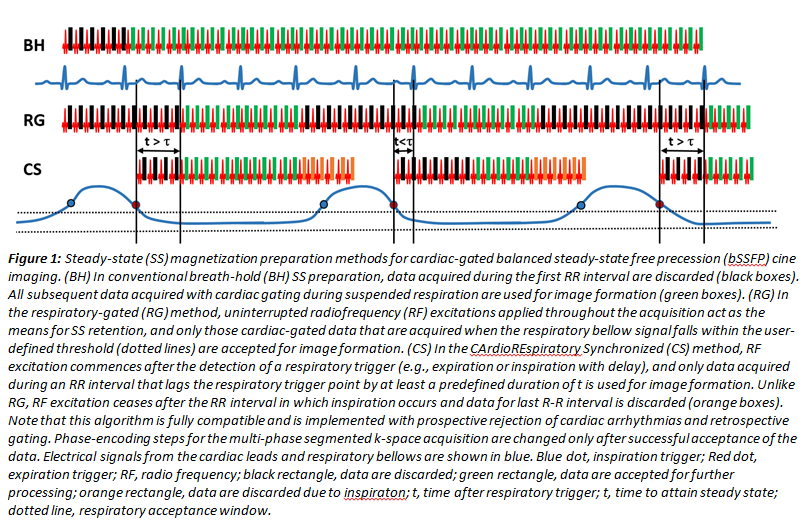
Figure 1: Steady-state (SS) magnetization preparation methods
for cardiac-gated balanced steady-state free precession (bSSFP) cine imaging.
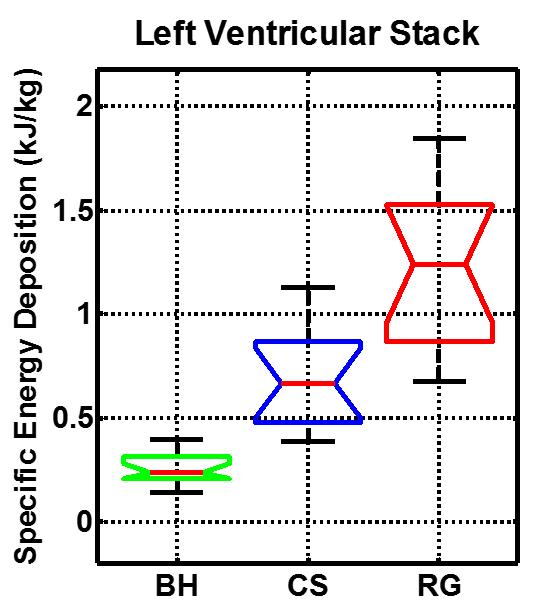
Figure 2: Total specific
energy deposition over the acquisition of entire left ventricular stack for BH,
CS and RG cine bSSFP sequences with identical acquisition parameters.
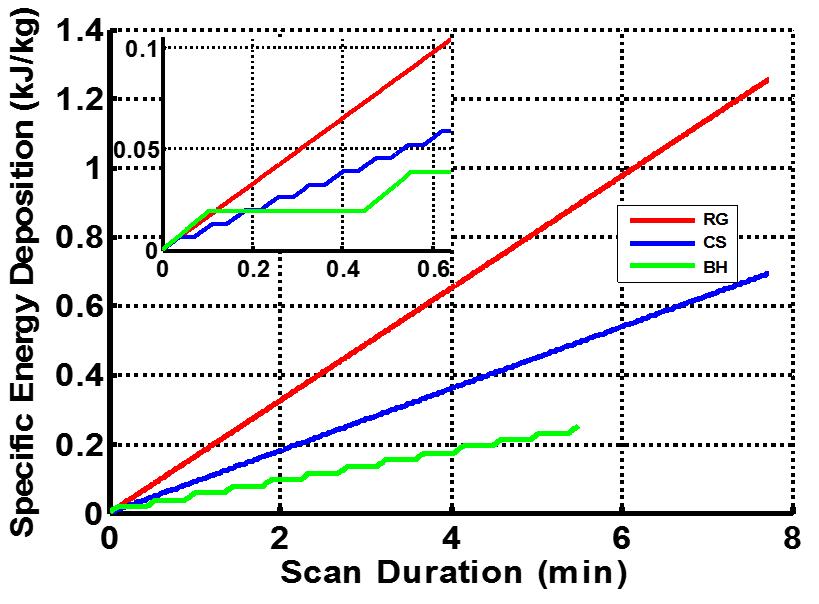
Figure 3: Cumulative specific energy deposition over the
acquisition of entire left ventricular stack for BH, CS and RG cine bSSFP
sequences with identical acquisition parameters (mean over 14 clinical patients).