2879
3D Stack-of-Stars Cardiac Cine MRI: Free-Breathing vs. Respiratory Gated Reconstruction1Internal Medicine II, University Hospital of Ulm, Ulm, Germany, 2Department of Cardiology, Zhongda Hospital, Medical School of Southeast University, Nanjing, People's Republic of China
Synopsis
3D cardiac cine MRI provides consistent data for complete LV analysis in a single scan. As this acquisition is too long for a breathhold, respiratory gating is typically applied.
The aim of this study is to investigate whether respiratory gating is also required for 3D cardiac cine MRI when using a Stack-of-Stars acquisition.
Ungated and Self-Gated reconstructions are compared visually and for LV function parameters.
As no motion artifacts are apparent even in the ungated cine data, and LV function results are comparable to the gated images, ungated reconstruction seems to be feasible for LV analysis.
Purpose
The intrinsic properties of radial acquisitions schemes have indicated a less relevant impact on quantitative parameters derived from free-breathing data without respiratory gating [1]. In this work, the impact of respiratory gating on derived global function parameters is investigated for an efficient hybrid radial-Cartesian 3D Stack-of-Stars Cine MRI technique.Methods
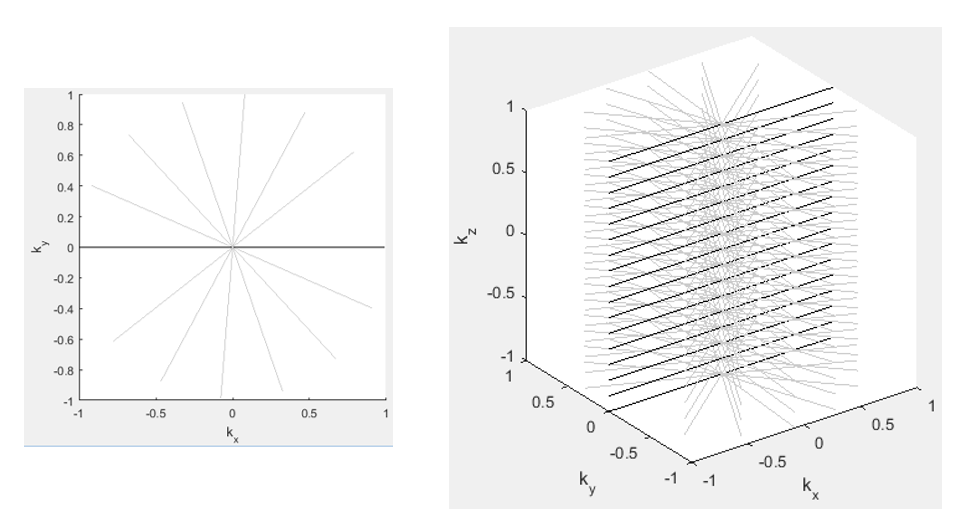
Six healthy volunteers (32±11 yrs) were enrolled in this study. All data were acquired with a 1.5 T whole-body scanner (Achieva 1.5T, Philips Healthcare, Best, The Netherlands) applying a hybrid radial (in-plane)-Cartesian(through-plane) 3D balanced acquisition in short axis orientation (see Figure 1). All k-space profiles for a given angle were encoded along the z direction first, before switching to the next angle [2]. Angular increment was set to the Tiny Golden Angle Ψ7≈23.628° [3] to ensure good k-space coverage even after resorting the data for cine reconstruction. Imaging parameters were as: resolution = 2x2x6 mm3, TE/TR = 1.2/2.4 ms, flip angle = 37°. Data was acquired continuously for 3:19 min:sec.
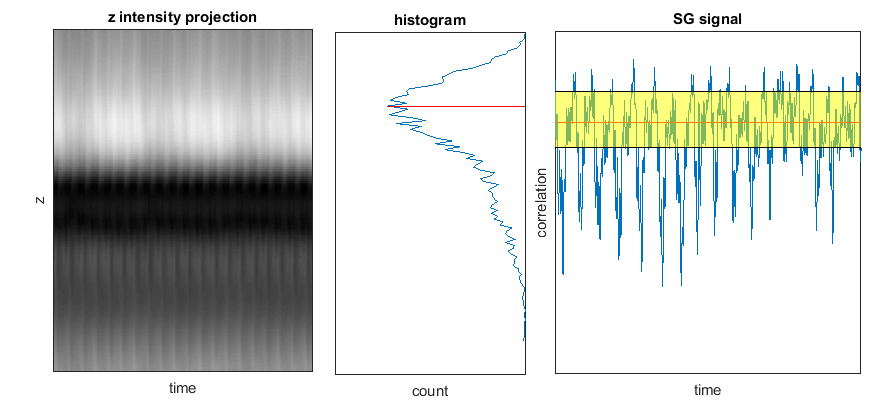
Reconstruction was performed using an in-house developed reconstruction package implemented in Matlab (Natick, MA, USA). Data were sorted into 20 cardiac phases according to the ECG signal recorded simultaneously during data acquisition. Ungated reconstructions were performed using all acquired data (100% efficiency). For the respiratory gated reconstruction, the image projection along the z direction (ZIP = z intensity profile) was used as input for selection of 50% of the acquired data (see Figure 2) in expiration [2]. To avoid any impact of the regularization required in iterative reconstruction methods, a simple gridding reconstruction was performed. To reduce resulting streaking artifacts, a weak TV-filter was applied before data analysis.
Left-ventricular (LV) function analysis was performed with Segment (Medviso, Lund, Sweden) [4], and compared between both reconstructions.
Results
All data were reconstructed successfully. Undersampling factors were 1.5±0.1 (ungated) and 3±0.2 (gated).
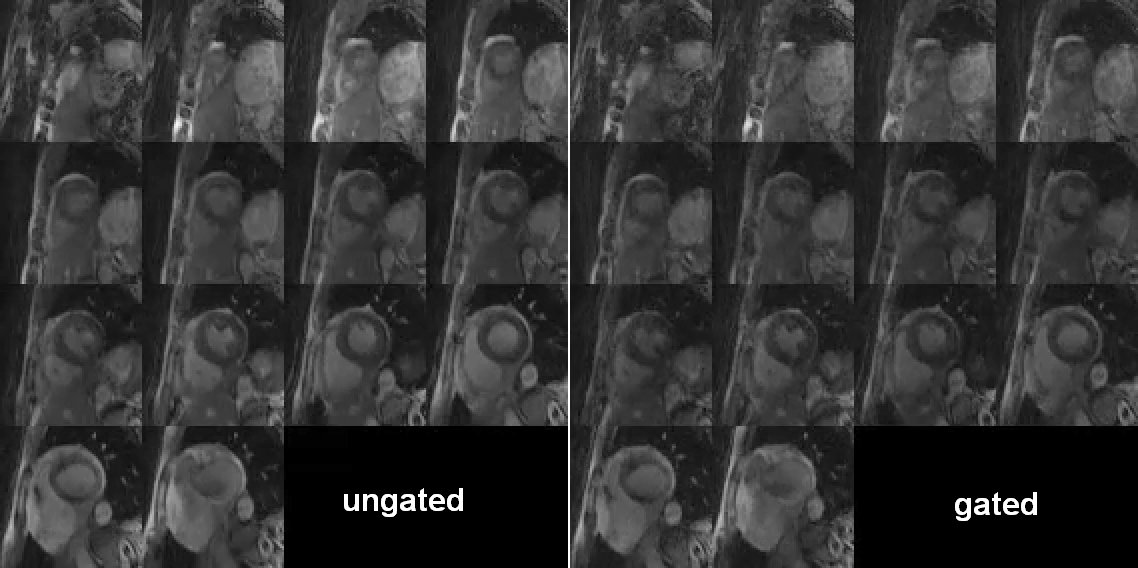
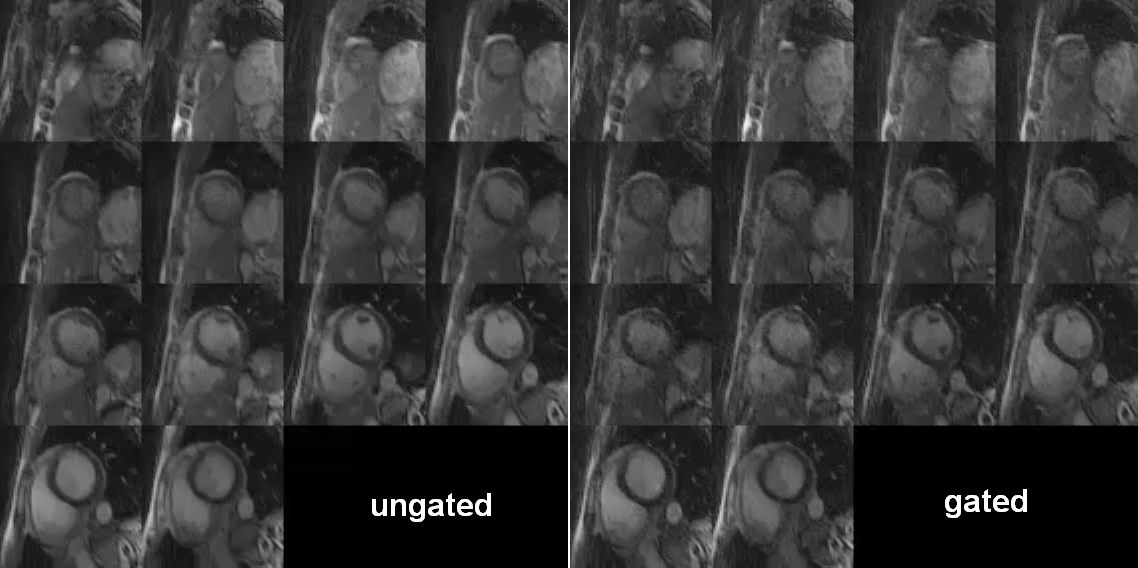
Figures 3 and 4 show a direct comparison for the ungated and gated reconstruction in end-systolic and end-diastolic cardiac phase, respectively. In neither reconstruction obvious motion artifacts like ghosting or blurring are apparent. A slight increase of undersampling streaking artifacts can be observed for the gated reconstruction due to the increased under-sampling.
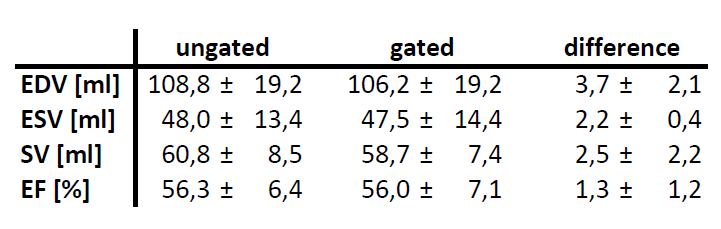
Comparison of LV functional parameters (see Figure 5) reveals highly similar values in both reconstructions, well below the standard deviation.
Discussion
In neither reconstruction, motion-related image artifacts were apparent and visual differences appear limited to increasing streak artifacts in the gated reconstruction due to the increased under-sampling. This, again, indicates the excellent intrinsic motion artifact properties of radial acquisition techniques. Even though distinct ghosting artifacts are expected in the phase-encoding (z-)direction, no impact on the global LV-function parameters could be observed, indicating a negligible impact on respiratory motion. The option of using 100% of the acquired data for final image reconstructions yields a huge gain in efficiency for the hybrid approach.Conclusion
With hybrid radial acquisition, no respiratory gating seems to be required for 3D Cardiac Cine imaging, thus yielding 100% scan efficiency. Further acquisition speedup might be achieved by application of Cartesian SENSE along the z-axis, and Compressed Sensing (CS) reconstruction allowing for higher radial undersampling factors.Acknowledgements
No acknowledgement found.References
[1] Paul et al., Does Respiratory Motion Influence Tissue Phase Mapping Velocities?, ISMRM, #2585, 2015.
[2] Liu et al., Respiratory and cardiac self-gated free-breathing cardiac CINE imaging with multiecho 3D hybrid radial SSFP acquisition. MRM, 63: 1230–1237. doi:10.1002/mrm.22306, 2010.
[3] Wundrak et al., A small surrogate for the golden angle in time-resolved radial MRI based on generalized fibonacci sequences, IEEE TMI, 34 (6), 1262-1269, 2015.
[4] Heiberg et al., Design and Validation of Segment – a Freely Available Software for Cardiovascular Image Analysis, BMC Medical Imaging, 10:1, 2010.
Figures