2876
3D left atrial strain imaging based on multi-slice radial cine and feature tracking1Yale University, New Haven, CT, United States
Synopsis
Left atrial (LA) strain is an important marker of left atrial remodeling. Two-dimensional atrial strain has been studied using echocardiography and MRI cine. Here we develop a 3D strain method, using volumetric cine data sets at multiple phases. The volumes were registered and 3D strain maps were generated, demonstrating patterns of regional strain in the LA.
Introduction
Left atrial (LA) strain is an increasingly recognized biomarker of left atrial remodeling, in patients with and without atrial fibrillation (AF) (1-5). Although myocardial tagging is not possible in the left atrium, feature tracking (6) with both echocardiography (1) and MRI cine (2-5) show lower left atrial strain in patients with atrial remodeling and AF. Most utilized methods are 2D, with long-axis views; they report global values. Our goal is to develop a volumetric atrial cine technique for 3D visualization of regional atrial strain. We hypothesize that this might provide complementary information on atrial remodeling, beyond that of atrial EF, volume, and LGE enhancement.Methods
Imaging: Healthy subjects (age 29±5) were scanned on a 3T scanner (Siemens Trio), using a 32-channel cardiac coil (Invivo, Pewaukee, WI), after providing informed consent. A multi-slice 2D GRE radial cine sequence was used to cover the entire LA and pulmonary veins within one breath-hold <25 seconds. The sequence parameters were: GRE, 300mmx300mm FOV, transverse view, 14-16 slices, 3mm slice thickness, 20% inter-slice distance, 1.9x1.9 in-plane resolution, 17 views per segment, 2 shots/slice, TR/TE/flip=6.1ms/2ms/12°. 401 Hz/pixel bandwidth, flow compensation. The projection angle of the radial trajectory was interleaved between adjacent cardiac phases to enable UNFOLD in the reconstruction to reduce artifacts due to undersampling. The k-space data was firstly reconstructed with parallel imaging (conjugate gradient SENSE) and then temporally filtered using UNFOLD. The multi-slice image set was interpolated to 1.8mm in the slice direction by zero padding the Fourier transform.
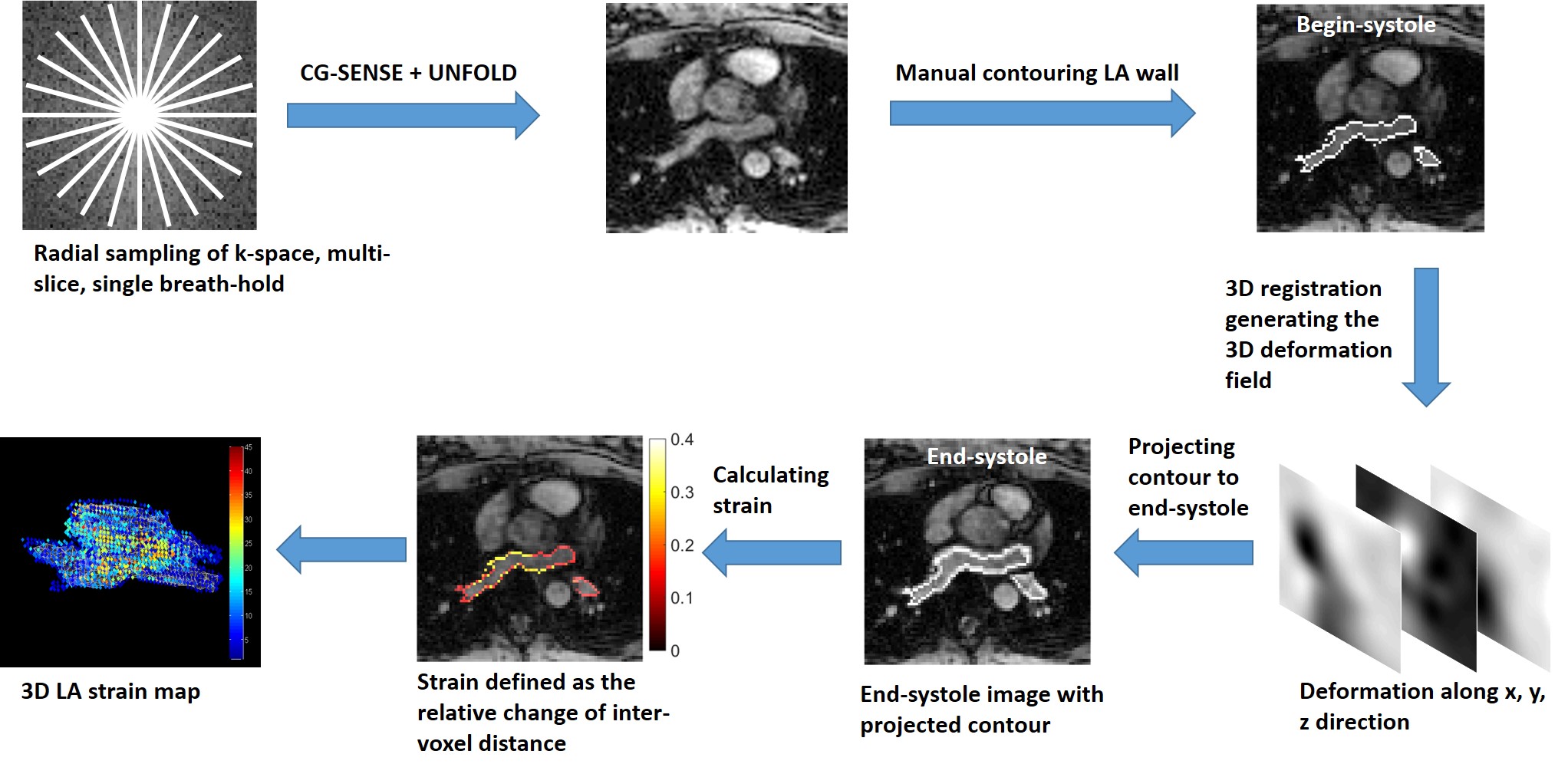
Analysis: Figure 1 shows the entire processing workflow. The 4D data was input into a non-rigid 3D registration algorithm (7) to calculate the displacement of each voxel in the first phase to subsequent phases. A strain map with intensity representing the magnitude of strain in each voxel was then generated using following steps: 1) the contour of LA in the begin-systolic phase was manually labeled. 2) For each voxel on the LA contour, all of its neighboring voxels and their projected positions in the end-systolic phase were localized based on the deformation field generated by the 3D registration algorithm. 3) The distance between the voxel and each neighboring voxel in both begin-systolic and end-systolic phases are measured, and the relative change of inter-voxel distance is calculated. The magnitude of the strain of each voxel is defined as the average of the relative change of distance between the voxel and its neighbors.
Results
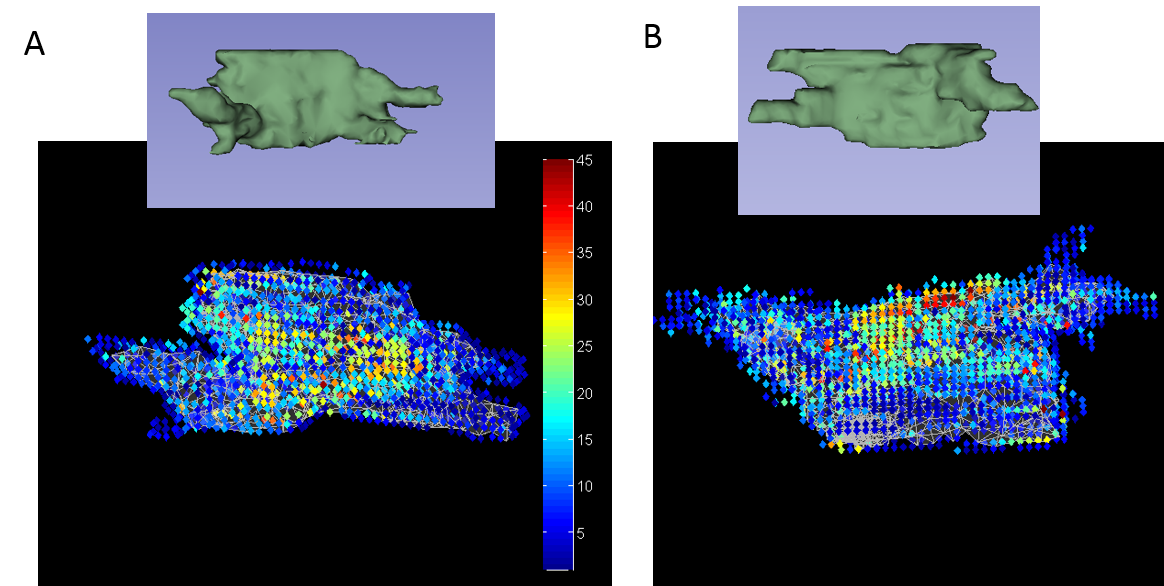
Figure 2 shows representative images of LA in the begin-systolic and end-systolic phases and the systolic expansion of LA. Figure 3 shows the 3D strain maps generated with the feature tracking algorithm, in two subjects. The average strain of the entire LA including part of pulmonary veins (PV) was 11%±1%, and peak strain in the LA was 52%±8%.Discussion and Conclusion:
We demonstrate the feasibility of a 3D feature-tracking based method for measuring left atrial regional strain. The multi-slice gradient-echo radial cine sequence is able to provide isotropic resolution and sufficient quality for the 3D registration algorithm. Although 3D and balanced SSFP methods provide higher SNR and shorter TRs, in the left atrium off-resonant spins reduce the quality of SSFP images (8), and three-dimensional cine has reduced inflow contrast. The average strain is lower than usually reported, because it includes strain from the entire atrium, e.g. the PV antrum. The assessment of reegional strain may provide more information on atrial remodeling than left atrial function or volume , or global strain. Atrial strain can potentially be or complementary to or even a surrogate of atrial fibrosis imaging, in assessment of atrial remodeling.Acknowledgements
No acknowledgement found.References
1. Kupphally SS et al. Radiology 2007. 2. Kowallick JT et al. JCMR 2014, 3. Habibi M et al. Circ Cardiovasc Imaging 2015,4. Evin M et al. JMRI 2015, 5. Peters DC et al. JACC Imaging 2016. 6. McEachen JC, et al. IEEE Trans Med Imaging, 1997. 7. Rueckert et al, IEEE Trans Medical Imaging 1999. 8. Hu P et al. JMRI 2010.Figures