2875
Global and regional wall motion abnormalities detected using strain-encoded MRI in comparison with late gadolinium enhancement in patients with sarcoidosis1Hokkaido University Graduate School of Medicine, Sapporo, Japan, 2Hokkaido University Hospital, 3Hokkaido University, 4Hokkaido University Graduate School of Medicine
Synopsis
We investigated global and regional myocardial wall motion abnormalities using strain-encoded (SENC) MRI in comparison with late gadolinium enhancement (LGE) in patients with systemic sarcoidosis. Fourteen patients were retrospectively evaluated. We found that global strain assessed using SENC MRI correlated well with global left ventricular (LV) dysfunction and the extent of LGE. In addition, regional longitudinal strain significantly decreased in segments with >10% LGE. SENC MRI has the potential to detect global and regional LV dysfunction and to predict the extent of LGE.
Purpose
In patients with systemic sarcoidosis, late gadolinium enhancement (LGE) with cardiac MRI (CMRI) has been used to detect cardiac involvement1. Strain-encoded (SENC) MRI, which was proposed by Osman et al.2, involves a special modification to the MRI scanning software that enables quantification of myocardial tissue regional deformation resulting from cardiac motion. This technique allows objective color-coded evaluation of longitudinal strain (LS) and circumferential strain (CS). The usefulness of SENC MRI for left ventricular (LV) regional motion analysis in ischemic heart diseases has been reported3. Nakano et al. presented a case report of cardiac sarcoidosis, in which severely impaired regional LS markedly diminished after corticosteroid therapy4. However, no report has discussed a relationship between LV wall motion abnormality and LGE in sarcoidosis. This study aimed to evaluate myocardial global and regional wall motion abnormalities using SENC MRI in patients with sarcoidosis and to evaluate its regional abnormality in comparison with LGE.Methods
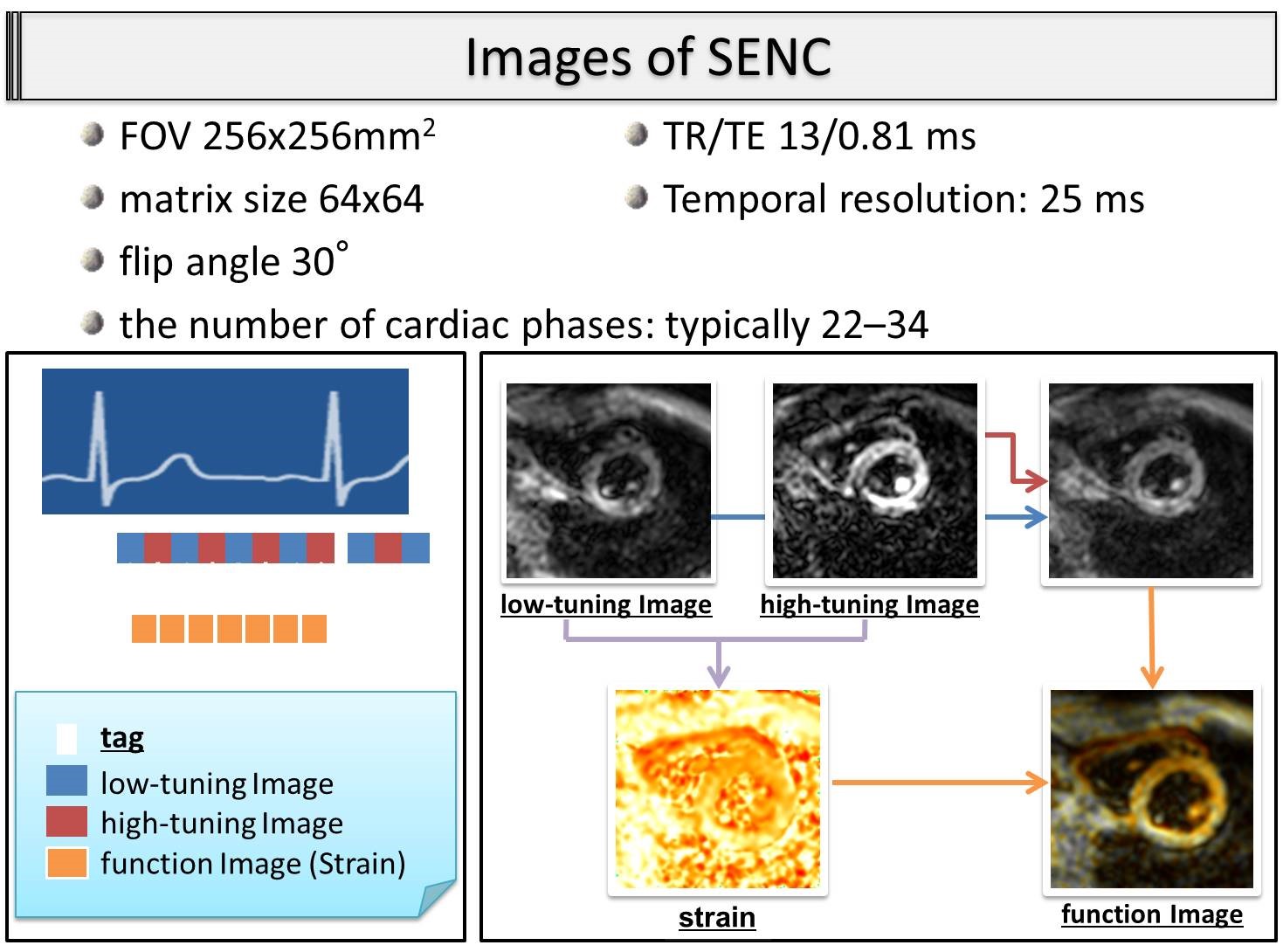
Our institutional review board approved this retrospective study and waived the requirement for informed consent. Fourteen patients with systemic sarcoidosis who underwent CMRI before any treatments were enrolled between July 2009 and July 2013. CMR was performed with a 1.5T Achieva system (Philips Medical System, Best, The Netherlands), equipped with a 5-element cardiac coil. In the fast SENC MRI sequence, the tagging gradient was applied in the slice-selection direction, orthogonal to the imaging plane. The fast SENC MRI parameters are shown in Fig. 1. LGE-CMRI was performed 10 minutes after administration of Gd-DTPA (0.1 mmol/kg, Magnevist; Berlex Laboratories, Wayne, NJ) with an inversion-recovery prepared, 3-dimensional fast-field echo pulse sequence. Myocardial strain was defined as the percentage change in tissue length occurring at peak systole (L) with respect to the initial resting length at end diastole (L0) [Strain = (L-L0)/L0]. Regional function was evaluated as the peak strain value at each point at the time of peak systolic contraction, using a dedicated software (Diagnosoft MAIN version 2; Diagnosoft Inc., Palo Alto, CA). The regional LS was evaluated in accordance with the American Heart Association 16 segmentation (Fig. 2). For CS, six regions of interest were selected in the septal and lateral walls at the basal, mid-ventricular, and apical levels (Fig. 2). For each global strain, average values of the peak 16 regional LSs and 6 regional CSs were calculated (LSgrobal and CSgrobal). The extent of LGE was quantified as the percentage of the myocardium (LGE%) with a CMR signal intensity ≥5 standard deviations (SDs) above the mean for the CMR signal intensity in the remote myocardium5. Endocardial and epicardial borders were semi-automatically traced from a stack of LV short axis cine images by a single expert radiologist using View Forum (Extended MR Work Space: ver. 2.6.3; Philips Medical Systems, Amsterdam, Netherlands) to obtain the LV mass (LVM) and ejection fraction (LVEF). Pearson’s correlation coefficient analyses were used to assess the relationship between global strain, LGE%, and LVEF. Differences in regional LS among segments with different degrees of LGE were assessed using one-way ANOVA. All statistical analyses were performed using JMP 12.0.1 (SAS institute, Cary, NC).Results
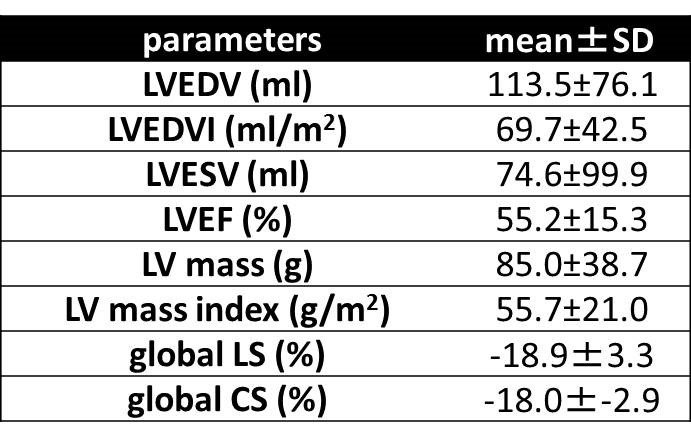
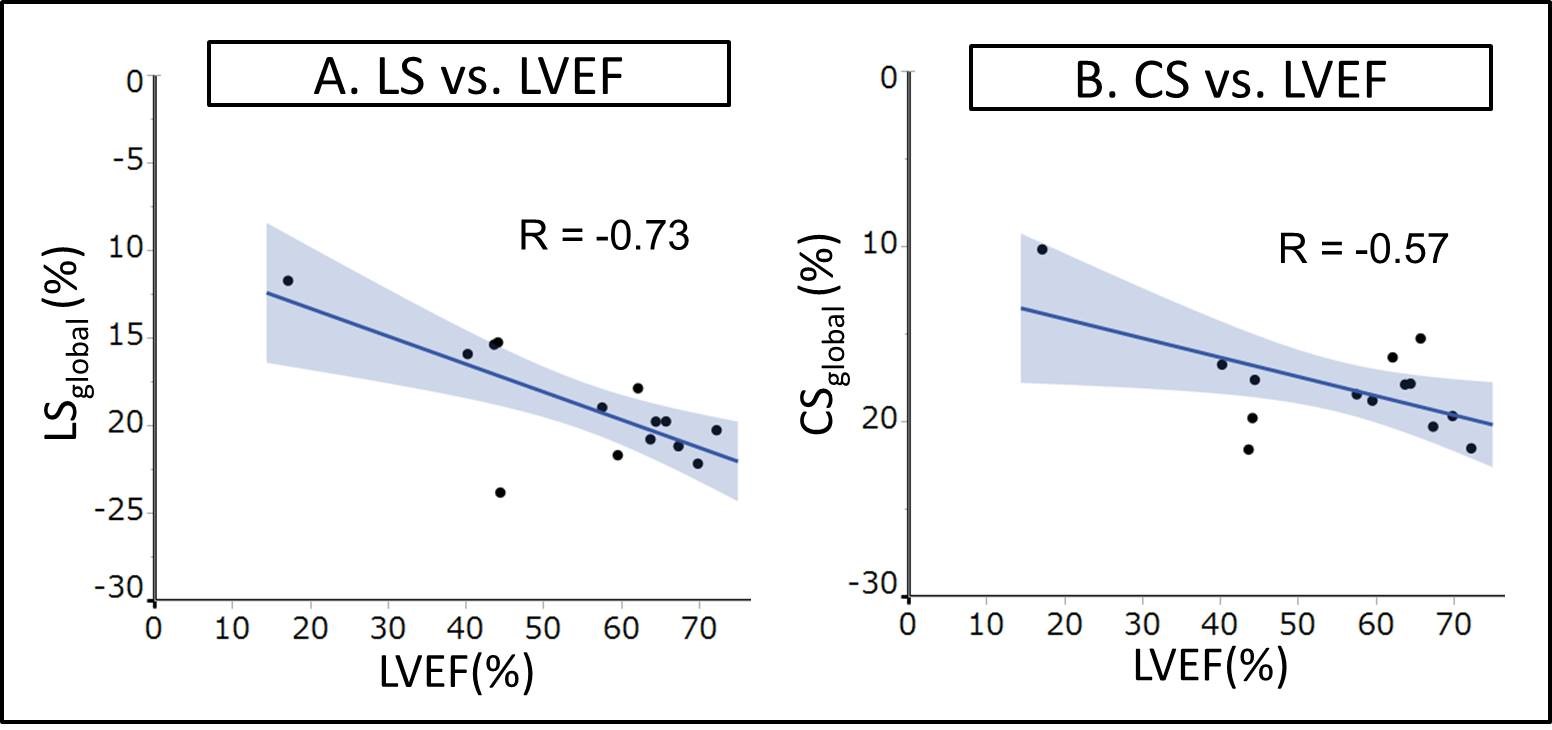
In total, 224 segments were assessable for LGE and strain analyses. LV volume analyses and global strains are summarized in Fig. 3. For the regional LGE analysis, 45 segments showed LGE in >10% of each myocardial segment, while 179 segments showed LGE in <10% of each segment. LSgrobal and CSgrobal showed significant correlations with LVEF (R=-0.73, P=0.003 and R=-0.57, P=0.03, respectively) (Fig. 4). CSgrobal showed a significant correlation with LGE% (R=0.62, P=0.01), while LSgrobal did not show a significant correlation (R=0.49, P=0.08). A representative case with inter-ventricular involvement is shown in Fig. 5. Regional LS was significantly lower in the segment with >10% LGE (-16.1±6.1%) than in that with <10% LGE (-19.6±5.3%, P=0.0009).Discussion
This is the first study to investigate regional and global myocardial wall motion abnormalities using SENC MRI in comparison with LGE in patients with sarcoidosis. We found that global strain determined using SENC MRI correlated well with LVEF and the extent of LGE. In addition, regional LS significantly decreased when the segment showed >10% LGE. Therefore, SENC MRI has the potential to detect global and regional LV dysfunction and to predict the extent of LGE.Conclusion
SENC MRI can potentially detect global and regional LV dysfunction and predict the extent of LGE in patients with sarcoidosis.Acknowledgements
NoneReferences
1) Smedema JP, Snoep G, van Kroonenburgh MP, et al. Evaluation of the accuracy of gadolinium-enhanced cardiovascular magnetic resonance in the diagnosis of cardiac sarcoidosis. J Am Coll Cardiol 2005;45(10):1683-1690.
2) Osman NF, Sampath S, Atalar E, Prince JL. Imaging longitudinal cardiac strain on short-axis images using strain-encoded MRI. Magnetic resonance in medicine 2001;46(2):324-34
3) Oyama-Manabe N, Ishimori N, Sugimori H, et al. dentification and further differentiation of subendocardial and transmural myocardial infarction by fast strain-encoded (SENC) magnetic resonance imaging at 3.0 Tesla. Eur Radiolo 2011;21(11):2362-8.
4) Nakano S, Kimura F, Osman N, et al. Improved myocardial strain measured by strain-encoded magnetic resonance imaging in a patient with cardiac sarcoidosis. Can J Cardiol. 2013 Nov;29(11):1531.e9-11.
5) Murtagh G, Laffin LJ, Beshai JF, et al. Prognosis of myocardial damage in sarcoidosis patients with preserved left ventricular ejection fraction: risk stratification using cardiovascular magnetic resonance. Circ Cardiovasc Imaging 2016;9(1):e003738.
Figures

Strain measurement
A total of 16 regional longitudinal strains and 6 circumferential strains are measured.
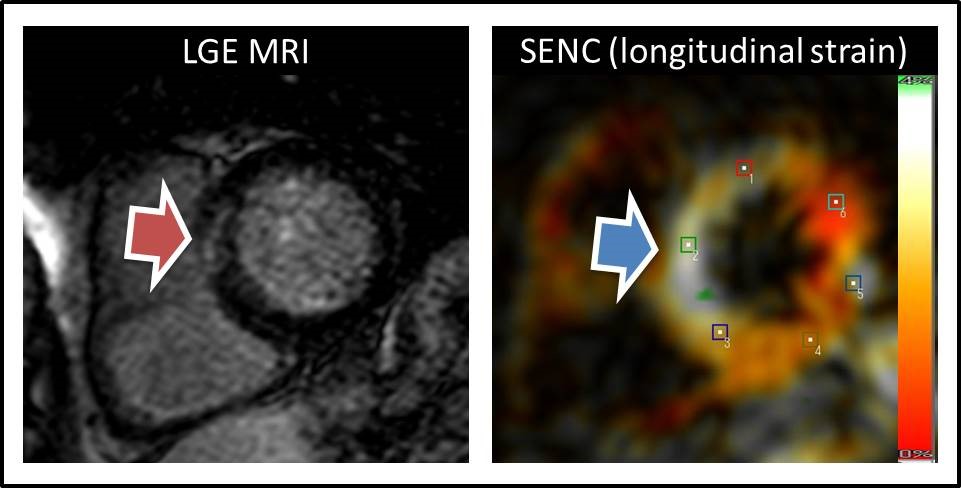
A representative case with inter-ventricular involvement
The left image shows late gadolinium enhancement (LGE) in the inter-ventricular septum (arrow). The right image (strain-encoded [SENC] MRI image) shows decreased regional strain (arrow), which is shown in white.