2870
Evaluation of left ventricular (LV) geometric models for estimating LV volumes in 980 children using cardiac cine magnetic resonance imaging1Diagnostic and Interventional Radiology, CHI St Luke's Health, Houston, TX, United States, 2Center for Coronary Artery Anomalies, Texas Heart Institute, Houston, TX, United States, 3Philips Healthcare, Cleveland, OH, United States
Synopsis
The results from this study that included cine SSFP images of the LV from 980 children show that LV volumes computed using commonly used bi-plane and tri-plane ellipsoidal models deviate significantly when compared to LV volumes estimated from a stack of short axis slices. A cut-cone+cone model of the LV proposed in this manuscript can estimate metrics describing LV function (EDV, ESV, and EF) with just two projections that are comparable to that obtained from an entire stack of short-axis slices.
Introduction
Unlike ultrasound and x-ray angiographic methods which estimate LV volumes based on a few select projections by making geometric assumptions about the shape of the LV, cardiac MR (CMR) based evaluation of LV volumes require no such assumptions, and with multi-slice, multi-phase CMR images of the heart it is possible to estimate LV volumes with high accuracy and precision1,2. However, these acquisitions are time consuming, and it is unknown if LV volumes estimated from a sub-set of projections (to reduce acquisition time) could provide estimation of LV volumes that are comparable to a fully sampled dataset.
In this study, we evaluate the performance of two commonly used models (bi-plane and tri-plane) for approximating LV with two and three projections to estimate LV volumes and compare them to LV volumes estimated from a fully sampled dataset. We propose three new models that can estimate LV volume with as few as two projections.
Materials and Methods
Patient Population: Data acquired from 980 school kids (recruited as a part of an IRB approved sudden cardiac death screening study) with no known history of heart disease (578 male, age: 12.6 ± 1.1 years) were used in this analysis.
MRI acquisition: VCG gated cine steady state free precession (SSFP) images of the LV (spatial resolution 2 x 2 x 8 mm3; temporal resolution < 50 ms) were acquired with in the short axis(SAx), left ventricular outflow tract (LVOT) and horizontal four chamber (4CH) orientations using a 32 Channel RF coil for signal reception.
Data analysis: Diastolic and systolic areas of the stack of slices in the short axis orientation encompassing the LV, as well as the long axis slices acquired in the LVOT and 4CH projections were measured by an expert observer. Furthermore, the cross sectional area of the short axis slice that included the dominant papillary muscle (Ap) was recorded. The length of the LV (measured from mitral annulus valve plane to the endocardium of the apex) from 4CH and LVOT orientations, as well as the diameter of the LV at the level of the mitral annulus in the 4CH and LVOT views were also recorded.
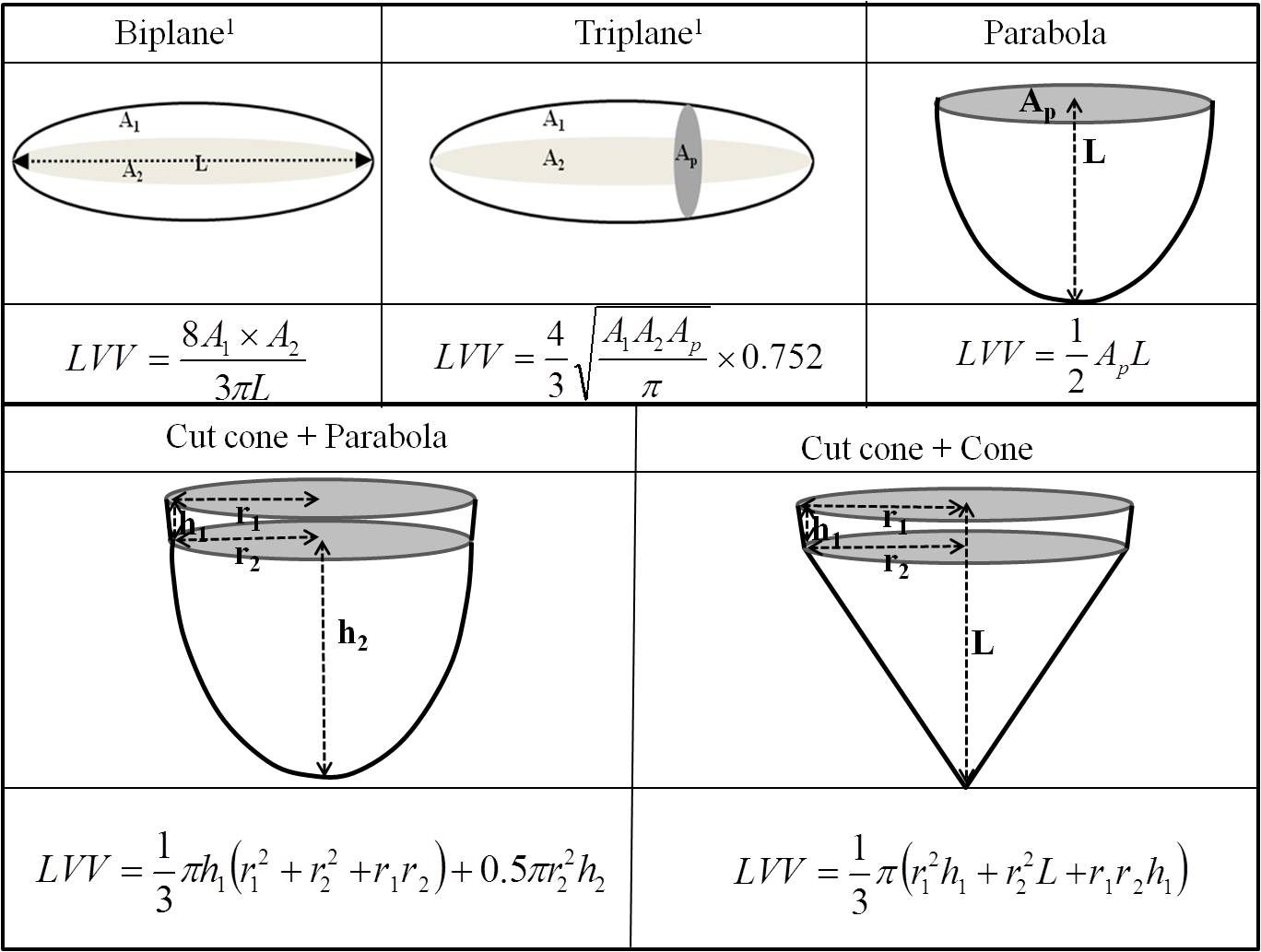
LV models: Five models to describe the shape of the LV are shown in Figure 1. Two commonly used biplane and triplane modes as well as the three other proposed models (parabola, cutcone+prabola and cutcone+cone) rely on a maximum of three projections.
Data analysis: Using LV volumes estimated from the stack of SAx as the reference, percentage-error and absolute difference of EDV, ESV, and EF of all five models were calculated and expressed as bias ± 1 standard deviation.
Results
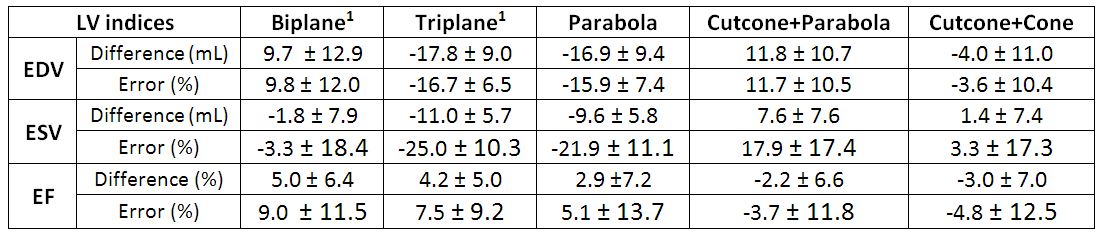
1. Biplane1 model of the LV overestimates EDV by 10% and triplane1 ellipsoid model underestimates EDV by 17%. With respect to ESV, biplane ellipsoidal model underestimates LV volume by 3%, and the triplane ellipsoidal model underestimates by 25%. With respect to EF, the biplane and triplane models overestimate by 9% and 8% respectively (Table 1).
2. Among the newly proposed model, the cutcone+cone model accurately estimates EDV, ESV and EF with least error.
Conclusions
1. In this large group of young children, our results show that the estimation of LV volumes using conventional geometric models such as bi-plane and tri-plane can result in significant errors.
2. Among the five models considered, Cutcone+cone model yields estimates of EDV, ESV and EF that are comparable to that obtained with a full stack of short axis slices with just two projections.
Acknowledgements
No acknowledgement found.References
1. Thiele, H et al. JCMR,4(3), 327-339,2002.
2. Malm, S et al. JACC, 44(5),1030-5,2004.
Figures