2857
Analysis of WSS variability subjected to changes of 4D flow parameters using a realistic aortic phantom.1Biomedical Imaging Center, Pontificia Universidad Católica de Chile, Santiago, Chile, 2Electrical Engineering Department, Pontificia Universidad Católica de Chile, Santiago, Chile, 3Radiology Department, School of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile, 4Hospital Virgen del Rocio, Universidad de Sevilla, Seville, Spain, 5Institute of Biomedicine of Seville, Universidad de Sevilla, Seville, Spain
Synopsis
The purpose of this work was to study the accuracy of the estimation of WSS calculated from 4D flow data acquired at different spatial and temporal resolutions. The data was acquired using a realistic thoracic aortic phantom in nine different hemodynamic conditions. We conclude that WSS measurements are more sensitive to changes in spatial resolution than in temporal resolution.
Purpose
To assess the variability of wall shear stress (WSS) as a function of 4D flow acquisition parameters. This assessment was done with a realistic phantom because it is difficult to perform on volunteers or patients. The acquisition of data sets is long (1), ranging from 5 to 30 minutes, so applying several sequences with different spatial and temporal resolution will lengthen the scanning time to more than 2 hours. Furthermore, by performing this study on volunteers it would be difficult to isolate the impact of spatial and temporal resolutions from other factors such as cardiac cycle variability and respiratory motion. In this work, we used a realistic thoracic aortic phantom to study the variability of WSS obtained from 4D flow data when subjected to changes of spatial and temporal resolutions in nine different hemodynamic conditions.Methods
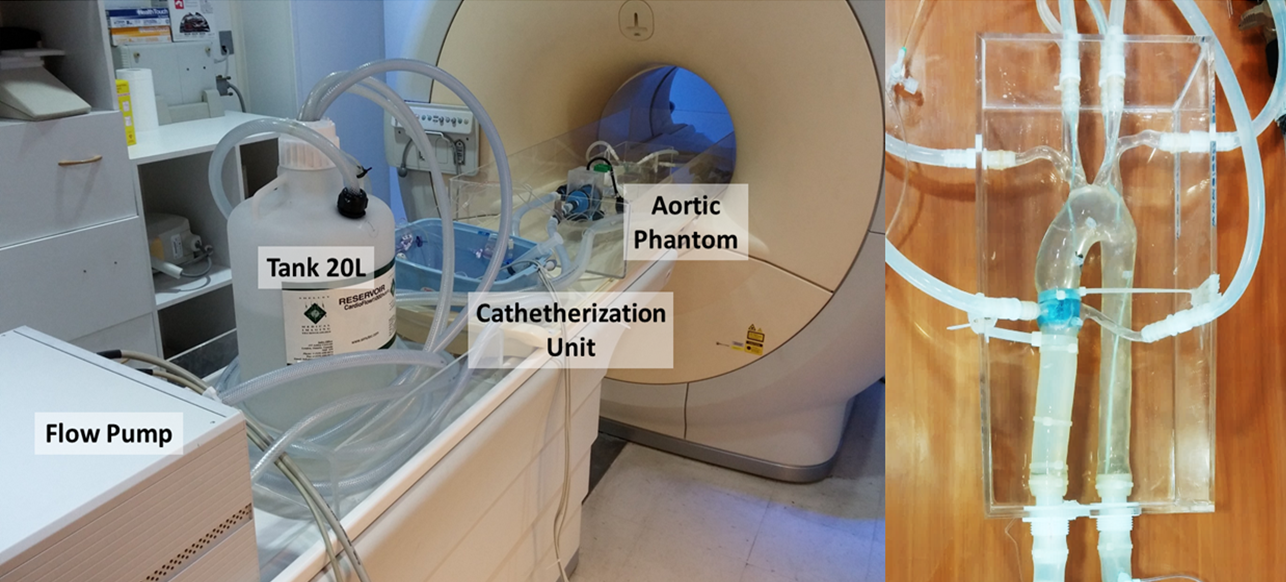
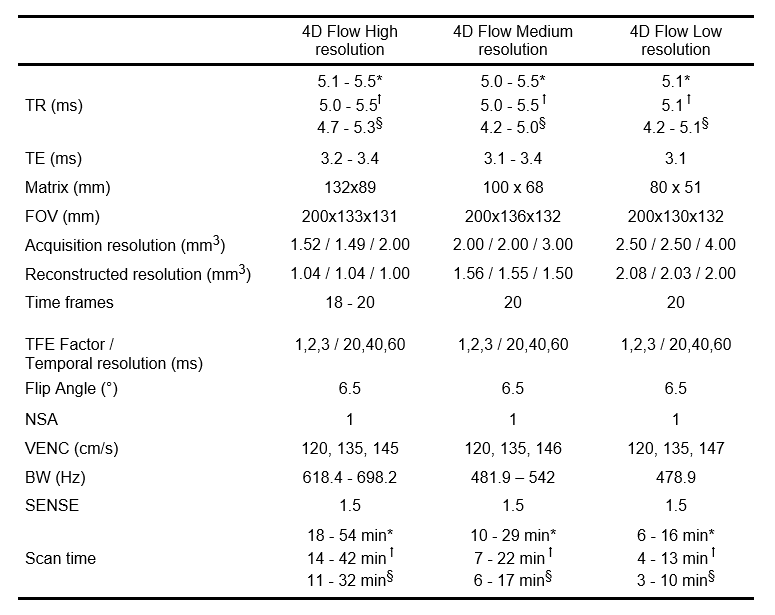
The experiments were performed using a Philips MR scanner (Achieva 1.5T, Best, Netherlands) with a 4-element phased-array body coil. The phantom model (T-S-N-005, Elastrat Sarl, Geneva, Switzerland) was equipped with a pulsatile MR-compatible flow pump (Simutec, London, Ontario, Canada), with the same features as explained by Urbina et al (2) (Figure 1). We controlled the pump in terms of flow waveform, heart rate and cardiac output, which allowed us to study nine different hemodynamic conditions: heart rates (HR) of 68, 88 and 115 bpm, and each one with different maximum flow rates (MFR) of 200, 230 and 260 ml /s. For each hemodynamic condition, nine 4D flow sequences were acquired in the entire phantom with different combinations of spatial (from 1.04 to 2.08 mm) and temporal resolutions (from 20 to 60ms cardiac phase). In total, we acquired eighty-one sequences of 4D flow data. All the MR acquisition parameters are summarized in Table 1.
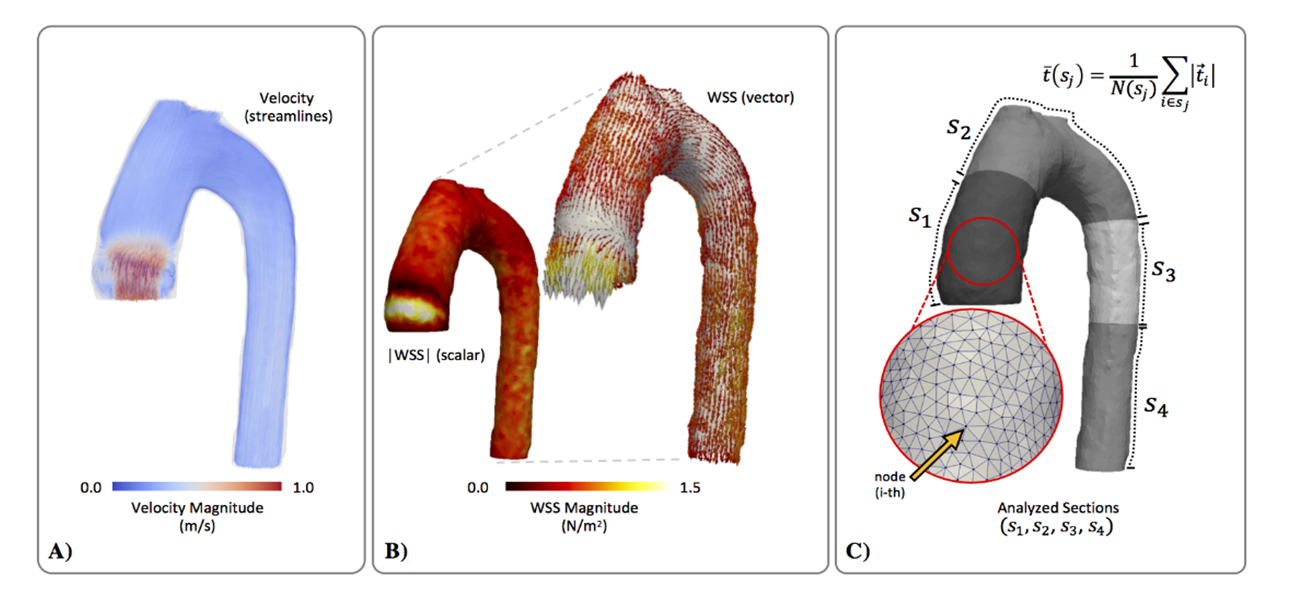
Mean WSS magnitude values were calculated for all 4D flow acquisitions. Since there is not a gold standard measurement for WSS, the 4D flow data with the highest combination of spatial and temporal resolution “HR20ms” (where the nomenclature: HR = highest spatial and 20ms =highest temporal resolution), was used for comparison. More nomenclature is shown in table 2. All 4D flow images were processed with a custom MatLab software toolbox. The quantification process included a semiautomatic segmentation of the aortic phantom and the generation of a tetrahedral finite element mesh, using the same method described previously by Sotelo et al (3). Different tetrahedral meshes were generated for each spatial resolution acquired.
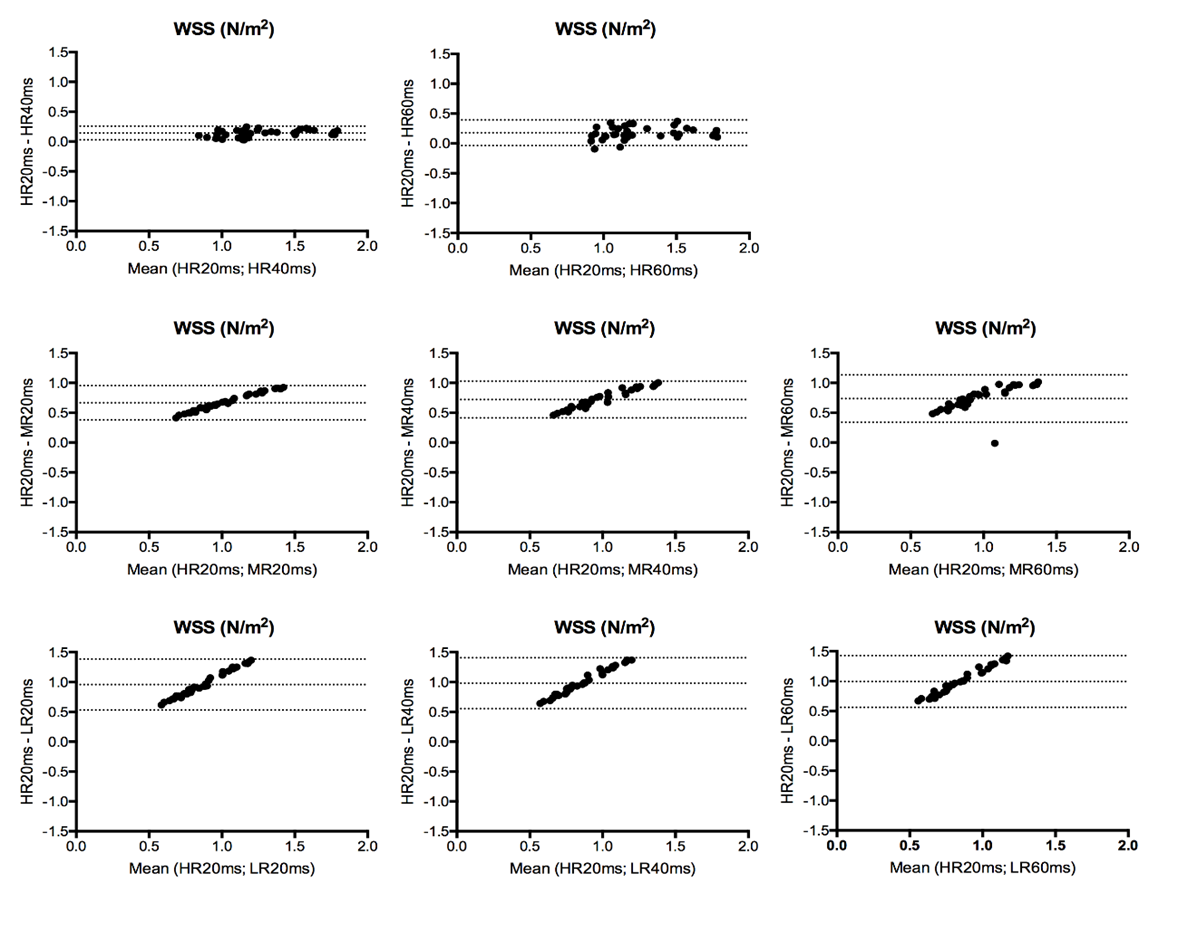
We analyzed the WSS magnitude values in four different sections of the aorta (Figure 2). Bland-Altman plots were created to describe the agreement of WSS values between all 4D flow data and the “gold-standard” HR20ms. Also, Mann-Whitney U test was used to assess statistical differences of WSS magnitude. Differences with P<0.01 were considered significant. The statistical analyses were performed using GraphPad Prism v.6 for Mac (GraphPad Software, La Jolla, CA).
Results
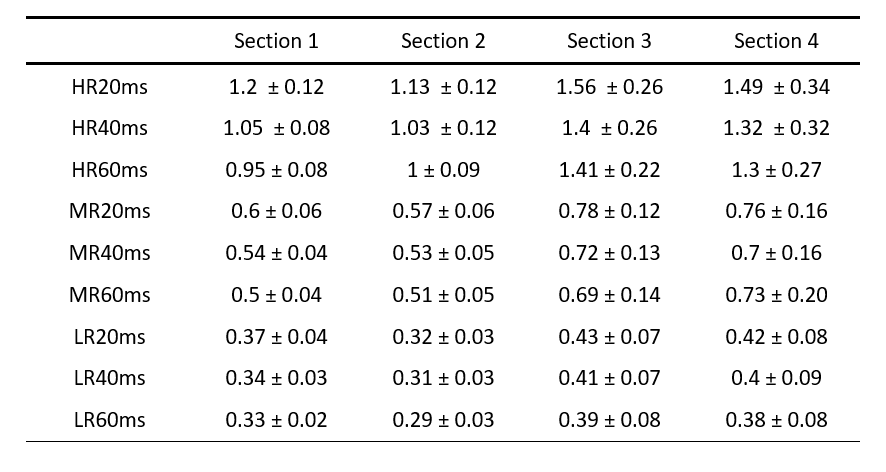
Table 2 shows the results of WSS magnitude values for all sections of the aorta. Highest variability was found in the acquisitions with low spatial resolution. We observed less differences when the acquisitions were subjected to changes in temporal resolution. In general, the results showed significant differences when comparing 4D flow data with HR20ms, except for the data acquired with high spatial and medium temporal resolution HR40ms (where the nomenclature: HR = highest spatial and 40ms = medium temporal resolution), no significant differences were observed for this case (p = 0.027). On the other hand, in the rest of acquisitions (shown in table 2) the results presented significant differences (p= <0.0001). These findings were corroborated on Bland-Altman analyses between 4D flow and HR20 (Figure 4).Discussion
In this study we demonstrated the effect of changes in spatial and temporal resolution on WSS magnitude measurements obtained from 4D flow acquisitions using a realistic aortic phantom. The WSS magnitude values were highly sensitive to changes of spatial resolution and less sensitive to changes of temporal resolution. The great advantage of this study is that we performed controlled experiments, avoiding any cardiac variability and respiratory motion. Statistical analysis demonstrated significant differences (p = 0.01) between HR20ms and in the most of 4D flow acquisitions with different combinations of spatial and temporal resolutions.Conclusion
Throughout controlled experiment using an aortic phantom we demonstrated that WSS magnitude values were highly sensitive to changes of spatial resolution and showed less variability when data was acquired with different temporal resolution.Acknowledgements
Grant Sponsor: Anillo ACT1416; Grant Sponsor: Fondo Nacional de Desarrollo Científico y Tecnológico (FONDECYT), Ministerio de Educación, Chile. Grant Number: FONDECYT #1141036.References
1. Cibis M, Potters W V, Gijsen F J, Marquering H, van Ooij P, vanBavel E, Wentzel J, Nederveen, A J. The Effect of Spatial and Temporal Resolution of Cine Phase Contrast MRI on Wall Shear Stress and Oscillatory Shear Index Assessment. Plos One. 2016;11(9), e0163316.
2. Urbina J, Sotelo JA, Springmüller D, Montalba C, Letelier K, Tejos C, Irarrázaval P, Andia ME, Razavi R, Valverde I, Uribe SA. Realistic aortic phantom to study hemodynamics using MRI and cardiac catheterization in normal and aortic coarctation conditions. J Magn Reson Imaging. 2016 Mar 10.
3. Sotelo J, Urbina J, Valverde I, Tejos C, Irarrázaval P, Hurtado DE, Uribe S. Quantification of Wall Shear Stress using finite-element method in multidimensional phase contrast MR data of the thoracic aorta. J Biomech. 2015;48:1817-1827.
Figures