2855
4D-Flow enables depictions and quantitative analysis of the characteristic flow fluctuations in the infrarenal aorta and diastolic suction flow in renal arteries1Radiology, Hamamatsu University School of Medicine, Hamamatsu, Japan, 2Department of Fundamental Development for Advanced Low Invasive Diagnostic Imaging, Nagoya University, Nagoya, Japan, 3Radiology, Stanford University School of Medicine, Palo Alto, CA, United States, 4Applied Science Laboratory Asia Pacific, GE Healthcare Japan, Hino, Japan
Synopsis
4D-Flow can be used to visually and quantitatively evaluate characteristic retrograde flow within the infrarenal abdominal aorta and the diastolic suction flow within the RAs, which might be the initiation factor of degradation of abdominal aortic wall followed by fatal aortic disease.
Purpose
Fusiform aneurysm is more commonly seen in abdominal aorta, especially at infrarenal portion; however, hardly seen in descending thoracic aorta.
We hypothesized that the characteristic flow dynamics within the infrarenal aorta may be affected by retrograde reflection wave from the iliac arteries and suction by renal arteries (RAs) during diastole. The retrograde flow increases oscillatory shear index (OSI) which reflects fluctuations of the directions of the wall shear stress (WSS) vectors. Previous physiological studies have shown that under higher OSI condition, the endothelium stimulates atherogenic drive (1).
3D cine PC MR imaging (4D-Flow) has enabled the full coverage of the spatial and cardiac phase resolved data of the velocity vectors of the flowing blood within the whole abdominal aorta, thereby allows quantitative flow volume measurement, calculation of the WSS and OSI as well as delineations of the streamlines at arbitrary sections in the abdominal blood vessels.
The purpose of our study is to quantitatively and visually analyze the characteristic blood flow dynamics that may make the infrarenal abdominal aorta prone to atherogenic fusiform aneurysm.
Materials & Methods
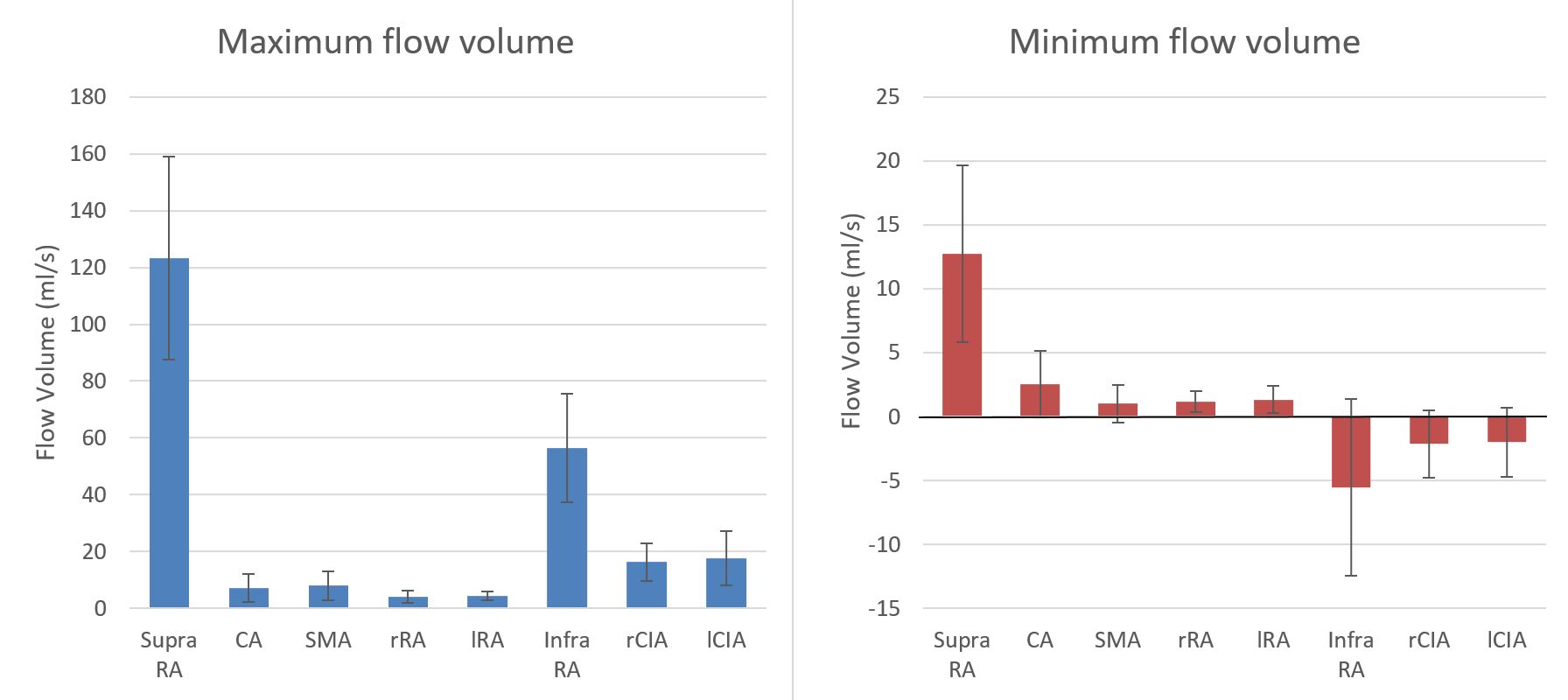
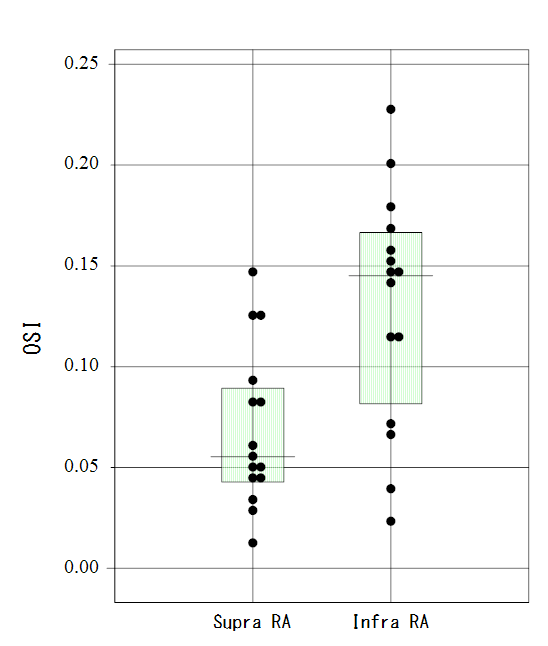
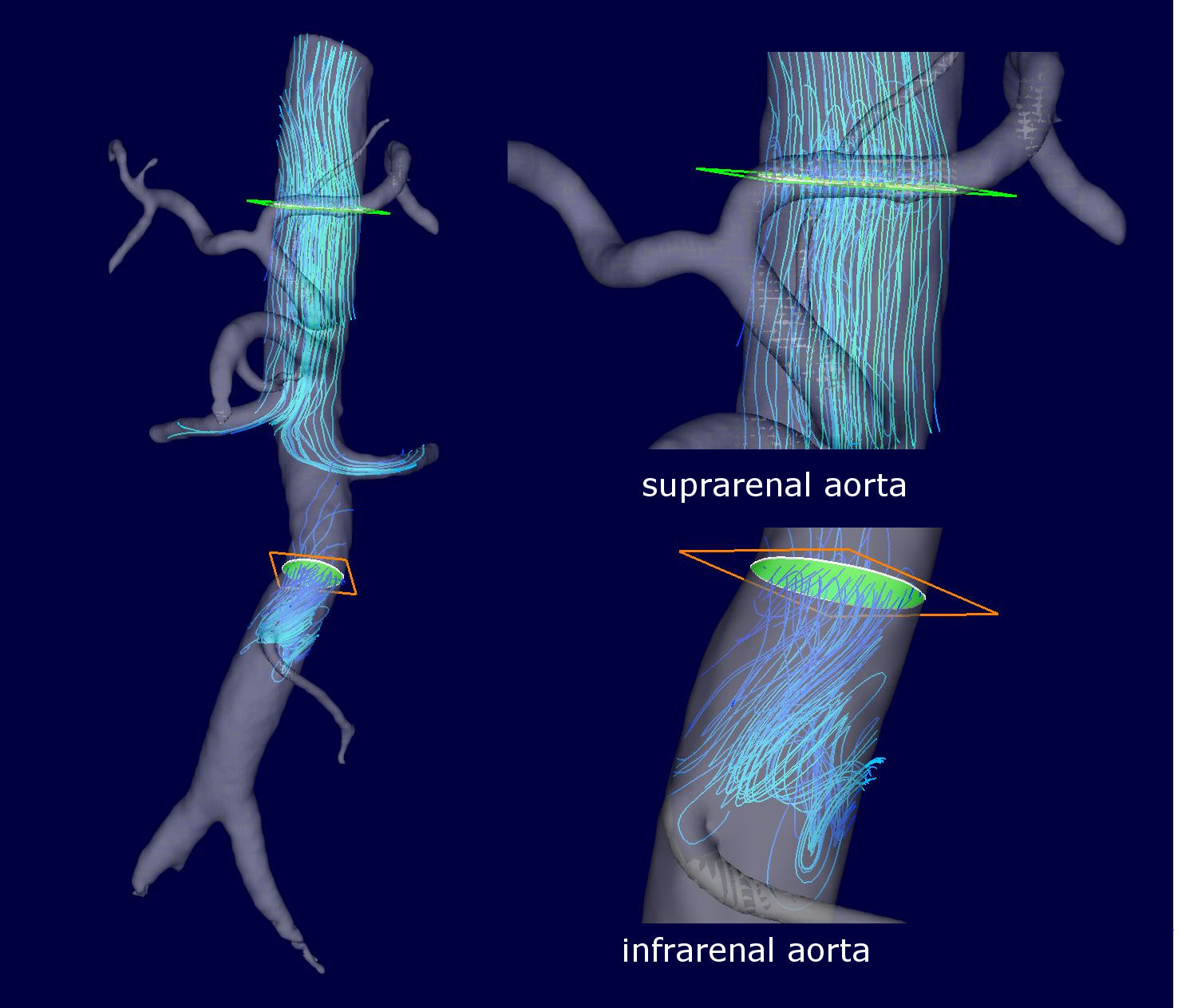
Between Mar 2013 and Sep 2014, fifteen consecutive patients (40 to 82 y.o.) who underwent MRI including abdominal 4D-Flow were enrolled in the study. The patients with remarkable aortic deformation such as aneurysm and tortuosity were excluded, because the scope of this study was to confirm the initial flow trigger of the atherogenic process, not the endpoint of the process. All the MR studies were conducted on a 3.0T MR imager with phased array coil. ECG gated, respiratory compensated gradient-echo-based coronal 4D-Flow covering from suprarenal abdominal aorta to bifurcation was performed following the contrast enhanced 3D MR Angiography (Gd3DMRA) performed for the determination of the aortic boundary. Acquired data were transferred to a workstation and were post-processed with flow analysis software (flova, R-tech, Japan). The velocity data derived from 4D-Flow and the geometric data of the boundary of the aortic wall determined by Gd3DMRA were interpolated. The maximum and minimum blood flow volume was measured at sections in supra and infrarenal abdominal aorta, celiac artery (CA), superior mesenteric artery (SMA), right and left RAs and common iliac arteries (CIAs). OSI within supra and infrarenal aorta were calculated and statistically compared by Mann-Whitney’s U test. Streamlines of supra and infrarenal aorta was delineated for streamline analysis.Results
8 male and 7 female patients were enrolled. The average minimal diastolic blood flow within suprarenal aorta was antegrade (12.73 +/- 6.92ml/sec), whereas that of infrarenal aorta was retrograde (-5.55 +/- 6.91ml/sec). The average minimal diastolic blood flow within RAs and other mesenteric arteries were antegrade. The average minimal diastolic blood flow of the CIAs was negative, reflecting the reflection flow waves. Streamlines within the infrarenal aorta depicted more turbulent flow than that of suprarenal aorta during diastole. The OSI of suprarenal aorta was significantly lower than that of infrarenal aorta (p<0.01, supraRA: 0.067 +/- 0.040, infraRA: 0.123 +/- 0.058).Discussion
The retrograde reflection flow might be characteristic within infrarenal aorta since RAs and other mesenteric arteries act as buffer that absorbs the reflection wave. The turbulence within infrarenal aorta was considered to be produced by the collision of the antegrade flow and the retrograde reflection flow. Turbulent flow caused by the retrograde flow within infrarenal aorta might be prominent factor for the development of fusiform aortic aneurysm following degradative change of abdominal aortic wall.Conclusions
4D-Flow can quantitatively and visually evaluate the blood flow dynamics within the abdominal aorta and the branching arteries in vivo non-invasively. The flow fluctuations in the infrarenal aorta may be triggering the degradation of the aortic wall followed by various fatal aortic disease.Acknowledgements
No acknowledgement found.References
1) Laughlin MH, J Appl Physiol. 2008 Mar;104(3):588-600.Figures